
17-13 TACTICAL COMBAT CASUALTY CARE VERSION 5 MAY 17

DIGITAL VERSION AVAILABLE
A digital version of this CALL publication is available to view or download
from the CALL website:
http://call.army.mil
Reproduction of this publication is welcomed and highly encouraged.
Tactical Combat Casualty Care
Handbook,
Version 5
FOLLOW CALL ON SOCIAL MEDIA
https://twitter.com/USArmy_CALL
https://www.facebook.com/CenterforArmyLessonsLearned

TACTICAL COMBAT CASUALTY CARE HANDBOOK
iii
Foreword
Tactical Combat Casualty Care (TCCC) has saved hundreds of lives during
our nation’s conicts in Iraq and Afghanistan. Nearly 90 percent of combat
fatalities occur before a casualty reaches a medical treatment facility.
Therefore, the prehospital phase of care is needed to focus on reducing
the number of combat deaths. However, few military physicians have had
training in this area and, at the onset of hostilities, most combat medics,
corpsmen, and pararescue personnel in the U.S. military have been trained
to perform battleeld trauma care through civilian-based trauma courses.
These courses are not designed for the prehospital combat environment and
do not reect current practices in the area of prehospital care. TCCC was
created to train Soldiers and medical personnel on current best practices for
medical treatment from the point of injury to evacuation to Role 3 facilities.
The challenge of meeting training needs was met by the voting members of
the Committee on Tactical Combat Casualty Care (CoTCCC) and its many
liaison members who collectively make up the TCCC Working Group. This
group includes trauma surgeons; emergency medicine physicians; internists;
family medicine physicians; operational physicians and physician assistants;
combat medical educators; trauma researchers; pathologists; combat
medical doctrine developers; medical equipment specialists; and combat
medics, corpsmen, and pararescue personnel. All the U.S. Armed Services
are well-represented in the TCCC Working Group’s committee membership,
and 100 percent of the CoTCCC voting members have been to war. The
CoTCCC and the TCCC Working Group represent different Services,
disciplines, and military experiences, all of which contribute to the single
goal of reducing preventable deaths on the battleeld.
This type of working group did not exist when the Twin Towers fell. The
U.S. Special Operations Command funded the initial group as a research
effort. Ownership of the group was then successively assumed by the
Naval Operational Medicine Institute, Defense Health Board, and, now, the
Joint Trauma System, which is part of the U.S. Army Institute of Surgical
Research.

iv
CENTER FOR ARMY LESSONS LEARNED
This group took the TCCC guidelines established in 2001 and continually
updated them. These updates were based on input from the Joint Trauma
System performance improvement trauma teleconferences, published case
reports and case series from war zones, breakthroughs in military medical
research, and new publications from civilian medical literature on combat
trauma. The group processed a continual stream of input from the battleeld
throughout the war years and ensured that battleeld trauma care lessons
were not only noted, but acted upon. So, they became lessons learned.
Through the efforts of this dedicated group of individuals, U.S. forces
have had prehospital trauma care guidelines customized for the battleeld
and updated continuously based on real-time evaluation of outcomes from
ongoing combat operations. This is the rst time in the nation’s history this
has occurred.
The success of the TCCC effort has been well-documented and is a great
tribute to all members of the CoTCCC and the TCCC Working Group. The
TCCC efforts transcend Service and medical specialty differences; expertly
process new information; and develop evidence-based, best-practice
guidelines that have completely transformed battleeld trauma care.
This TCCC Handbook is dedicated to the CoTCCC and all the valued
colleagues in the TCCC Working Group. Our country and its casualties owe
you all a profound measure of thanks.
Frank Butler, MD
CAPT (Retired), MC, USN
Chairman, Committee on
Tactical Combat Casualty Care

v
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Tactical Combat Casualty Care Handbook
Table of Contents
Chapter 1. Tactical Combat Casualty Care Overview 1
Hemorrahage Control 4
Airway Management 8
Breathing Management 19
Vascular Access 24
Hypothermia Prevention 40
Tactical Field Care Basic Management Plan 42
Chapter 2. Tactical Combat Casualty Care Phases of Care 45
Chapter 3. Tactical Combat Casualty Care Medical Equipment 53
Chapter 4. MARCH/PAWS Treatment Algorithms 63
Chapter 5. Tactical Combat Casualty Care-All Combatants 71
Chapter 6. Tactical Combat Casualty Care-Medical Provider 79
Appendix A. Tactical Combat Casualty Care Card 93
Appendix B. Tactical Combat Casualty Care After Action
Report
97
Appendix C. Medical Triage Categories 101
Appendix D. Medical Evacuation Precedence Categories 105
Appendix E. 9-Line Request With MIST Report 107
Appendix F. Prolonged Field Care 109
Appendix G. Drug Reference Guide 111
Appendix H. Medical Transition Guidelines in a Tactical
Environment
113
Appendix J. Tactical Combat Casualty Care Background 119
Appendix K. References 121

vi
CENTER FOR ARMY LESSONS LEARNED
Center For Army Lessons Learned
CALL Director COL Michael F. Pappal
CALL Analyst CPT Ryan St. Jean
Contributing Authors MAJ Walter Engle
Jonathan C. Fruendt, M.D.
The Secretary of the Army has determined that the publication of this
periodical is necessary in the transaction of the public business as required
by law of the Department.
Unless otherwise stated, whenever the masculine or feminine gender is
used, both are intended.
Note: Any publications (other than CALL publications) referenced in
this product, such as ARs, ADPs, ADRPs, ATPs, FMs, and TMs, must be
obtained through your pinpoint distribution system.

1
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Chapter 1
Tactical Combat Casualty Care Overview
Introduction
The Tactical Combat Casualty Care (TCCC) concept was developed in 1996
by special operations forces. Tactical Combat Casualty Care guidelines are
evidence-based and battleeld-proven to reduce deaths at the point of injury
(POI). Department of Defense (DOD) and NATO allies require TCCC
training for deploying forces because it combines effective tactics and
medicine.
TCCC-Medical Provider (TCCC-MP) is training for medical personnel.
TCCC-All Combatants (TCCC-AC) is training for rst responders and non-
medical personnel. TCCC training is performed in three phases: Care under
re (CUF), tactical eld care (TFC), and tactical evacuation care (TEC) (for
more information, see Chapter 2, Tactical Combat Casualty Care Phases of
Care).
TCCC teaches rst responders to treat casualties in the proper order, treating
the most critical situations rst. This is done using the acronyms MARCH
and PAWS (see below).
MARCH Acronym
MARCH (massive hemorrhage, airway, respirations, circulation, head
injury/hypothermia) is an acronym used by TCCC-trained individuals to
help remember the proper order of treatment.
Massive hemorrhage. The number one potentially survivable cause
of death at the POI is hemorrhage from a compressible wound or any
life-threatening extremity bleed. More than 90 percent of 4,596 combat
deaths post 11 September 2001 died of hemorrhage-associated injuries.
The hasty application of a Committee on Tactical Combat Casualty Care
(CoTCCC)-approved tourniquet is the recommended management for all
life-threatening extremity hemorrhages during care under re (see page 4).
It is initially placed over clothing, high and tight. The deliberate application
of a tourniquet is addressed when behind cover and during tactical eld
care to ensure proper hemorrhage control. The tourniquet is placed under
clothing 2 to 3 inches above the wound. The application time is written on
the tourniquet. Combat gauze is the hemostatic dressing of choice.

2
CENTER FOR ARMY LESSONS LEARNED
Airway. A second survivable cause of death at the POI is a non-patent
(closed) airway. Airway injuries typically occur from maxillofacial trauma
or inhalation burns. A conscious and speaking casualty has a patent open
airway. An unconscious casualty who is breathing can benet from the
nasopharyngeal airway (NPA) (see page 8). An unconscious casualty
who is not breathing may require a denitive airway such as a surgical
cricothyroidotomy (see page 11). In a combat setting, endotracheal
intubation is highly difcult, if not impossible.
Respirations. The third potentially survivable cause of death on the
battleeld is the development of a tension pneumothorax (PTX). Air
trapped in the chest cavity begins to displace functional lung tissue and
places pressure on the heart, resulting in cardiac arrest. Seal open chest
wounds with a vented chest seal, decompress a suspected PTX, and
support ventilation/oxygenation, as required. Treat a PTX via needle chest
decompression (NCD) using a 14-gauge, 3.25-inch-long needle with a
catheter (see page 20).
Circulation. Control of bleeding takes precedence over infusing uids.
Only individuals in shock or those who need intravenous (IV) medications
need to have IV access established. Use an 18-gauge catheter and saline
lock in a eld setting. Give tranexamic acid (TXA) as soon as feasible
to casualties in or at risk of hemorrhagic shock. Once a saline lock is
established, secure it with transparent wound-dressing lm. Administer
uids by a second needle and a catheter through the lm dressing. When the
infusion is complete, withdraw the needle, leaving the saline lock in place.
An intraosseous (IO) device is an alternative route for administering uids
when uid resuscitation is required and an IV access cannot be obtained.
Clinical signs of shock on the battleeld are: 1) unconsciousness or altered
mental status not due to coexisting traumatic brain injury (TBI) or drug
therapy; and/or 2) abnormal radial pulse.
Head injury/hypothermia. Hypotension (systolic blood pressure [SBP]
under 90) and hypoxia (peripheral capillary oxygen saturation [SpO2]
under 90) worsen secondary brain injury. Medical personnel identify
mild traumatic brain injury (mTBI) using the Military Acute Concussion
Evaluation (MACE) (more information on MACE is available online at
https://dvbic.dcoe.mil/material/military-acute-concussion-evaluation-
mace-pocket-cards). Non-medical personnel utilize the alert, verbal, pain,
unresponsive (AVPU) scale. Hypothermia is a survivable cause of further
injury and is dened as a whole body temperature below 95 F (35 C).
Hypothermia, acidosis, and coagulopathy constitute the lethal triad in
trauma patients. Hypothermia can occur secondary to blood loss, regardless
of the ambient temperature. The Hypothermia Prevention and Management
Kit (HPMK) is recommended by the CoTCCC for all casualties.

3
TACTICAL COMBAT CASUALTY CARE HANDBOOK
PAWS Acronym
PAWS (pain, antibiotics, wounds, splinting) is an acronym used by TCCC-
trained individuals to help remember additional casualty care issues.
As noted in the U.S. Central Command Joint Theater Trauma System
publication, Saving Lives on the Battleeld, Part I, 30 January 2013,
and Saving Lives on the Battleeld, Part II, 30 May 2014, a survey of
military personnel deployed showed that pain management, antibiotics,
splinting, and reassessing interventions and additional wounds were
often not performed. The PAWS acronym allows personnel to recall these
interventions while under duress.
Pain. Management of a casualty’s pain helps reduce stress on the mind
and body. By managing pain from the POI onward, casualties have
reduced incidents of post-traumatic stress disorder (PTSD) at Role 4 care
(rehabilitation) and beyond. Pain management reduces patient movement,
improves compliance and cooperation, and allows for better casualty
transport and outcomes.
Antibiotics. The recommended parenteral antibiotics for POI care are
ertapenem, 1 gram (gm); or cefotetan, 2 gm. These antibiotics are used
to treat multidrug-resistant bacteria. Ertapenem has been designed to be
effective against Gram-negative and Gram-positive bacteria. Cefotetan is
a second-generation cephalosporin and has a broad spectrum of activity; it
has been used to treat bacterial infections of the bone, skin, urinary tract,
and lower respiratory tract. Moxioxacin is a broad-spectrum quinolone
antibiotic that can be administered orally. If the casualty can tolerate
oral uids, moxioxacin, 400 milligrams (mg), can be given instead of
ertapenem of cefotetan. All battleeld wounds are considered contaminated.
All wounded casualties with penetrating injuries should receive antibiotics.
Wounds. Assessing and treating casualties with additional wounds
improves morbidity and mortality. Minor scalp lacerations can be the
cause of excessive hemorrhage. First responders must address burns, open
fractures, facial trauma, amputation dressings, and security of tourniquets.
Reassessment of wounds and interventions prior to movement is critical.
When preparing the patient for transport, casualties with penetrating trauma
to the chest or abdomen should be evacuated on an emergent basis, due to
the possibility of internal hemorrhage. Responders should give TXA as soon
as feasible to casualties in or at risk of hemorrhagic shock.

4
CENTER FOR ARMY LESSONS LEARNED
Splinting. Medical personnel should address pelvic disruptions and
eye injuries. The energy required to cause a lower extremity traumatic
amputation (from an improvised explosive device [IED], land mine,
etc.) moves upward through the body, potentially causing further bone
disruption, hollow organ collapse, or internal bleeding. Responders should
use the Combat Ready Clamp (CRoC), the Junctional Emergency Treatment
Tool (JETT), or the SAM Junctional Tourniquet to control junctional
hemorrhage and stabilize the pelvis. Splinting of fractures can result in
signicant pain relief and minimize bleeding.
In cases of suspected penetrating eye trauma, responders should: 1) perform
a rapid eld test of visual acuity; 2) tape a rigid shield over the eye to
prevent further trauma to the eye; and 3) give moxioxacin, 400 mg, by
mouth as soon as possible to prevent infection inside the eye. Never apply a
pressure dressing to an eye with a suspected penetrating injury.
Tactical Field Care
Tactical eld care is the backbone of TCCC. It is the how-to for utilizing
MARCH and PAWS to treat combat casualties. The following information
details how to properly execute tasks commonly associated with tactical
eld care basic management. The tasks are organized in the appropriate
order based on MARCH and PAWS.
Hemorrhage Control
(Addressed During Care Under Fire and Tactical Field Care Phases.
See Chapter 2, Tactical Combat Casualty Care Phases of Care, Page 45.)
Combat Application Tourniquet
Figure 1-1. Combat application tourniquet

5
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Step 1. During the care under re phase, place the tourniquet as high on the
extremity as possible and over the uniform. This is a hasty tourniquet. (This
will be transitioned to a deliberate tourniquet on the skin, 2 inches above the
injury in the tactical eld care phase.)
Figure 1-2. Step 1
Step 2. Route the self-adhering band through the friction adapter buckle.
Pull the band tight, removing all slack.
NOTE: Current TCCC doctrine says utilizing the single slot on a routing
buckle is effective. The Combat Application Tourniquet (CAT) Generation 7
(not yet widely elded) was redesigned with this feature.
Figure 1-3. Step 2

6
CENTER FOR ARMY LESSONS LEARNED
Step 3. Feed the self-adhering band tight around the extremity and securely
fasten it back on itself. No more than three ngers should t between the
band and the injured extremity.
Figure 1-4. Step 3
Step 4. Twist the windlass rod until the bleeding stops and the distal pulse
has been eliminated.
Figure 1-5. Step 4

7
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Step 5. Lock the windlass rod in place with the windlass clip.
Figure 1-6. Step 5
Step 6. Grasp the windlass strap, pull tight, and adhere it to the windlass
clip.
Figure 1-7. Step 6
Step 7. If the tactical situation permits, check for a distal pulse. If a distal
pulse is still present, apply a second tourniquet side by side and proximal to
the rst. Tighten this tourniquet and recheck the distal pulse.
Combat Gauze
1. Place the end of the combat gauze over the dominant hand, index nger.
Using this nger, place the combat gauze into the wound, directly at the
pulstating artery. Then, begin to pack the wound until it is full of the combat
gauze. (See Figure 1-8.) Place any excess combat gauze directly over the
wound and apply direct pressure for 3 minutes.
NOTE: More than one combat gauze may be required to completely ll the
wound. If bleeding continues after 3 minutes of pressure, rst remove the
combat gauze and repeat step 1.

8
CENTER FOR ARMY LESSONS LEARNED
NOTE: Attempt to visualize the bleeding during dressing transition. Look
for owing blood from veins or spurting blood from arteries. Attempt to
place the second combat gauze on the source of the bleeding.
2. Once bleeding is controlled, apply an outer bandage (Ace wrap or
emergency dressing) to secure the dressing to the wound.
Figure 1-8
Airway Management
(Addressed During Tactical Field Care and Tactical Evacuation Care Phases.
See Chapter 2, Tactical Combat Casualty Care Phases of Care, Pages 45 and 46.)
Nasopharyngeal Airway (NPA)
1. Place the casualty supine with the head in a neutral position.
Caution: Do not use the NPA if there is clear uid (cerebrospinal uid)
coming from the ears or nose. This may indicate a skull fracture.
2. Lubricate the tube with a water-based lubricant.
Caution: Do not use a petroleum-based or non-water-based lubricant.
These substances can cause damage to the tissues lining the nasal
cavity and pharynx, increasing the risk for infection.

9
TACTICAL COMBAT CASUALTY CARE HANDBOOK
3. Insert the NPA:
• •
Push the tip of the nose upward gently.
• •
Position the tube so the bevel of the airway faces toward the septum.
• •
Insert the airway into the nostril and advance it until the ange rests
against the nostril.
Figure 1-9
Caution: Never force the NPA into the casualty’s nostril. If resistance is
met, pull the tube out and attempt to insert it in the other nostril. Most
attempts to insert the NPA should be in the right nostril. If unable to
insert into the right nostril, try the left. If inserting in the left nostril, the
bevel will not be against the septum.
Nasopharyngeal Airway Training Skill Sheet
Objective: To demonstrate the recommended procedure for insertion of an
NPA.
References:
• •
Prehospital Trauma Life Support, Military Eighth Edition, Jones and
Bartlett Learning, November 2014
• •
Advanced Trauma Life Support Manual, Ninth Edition, American
College of Surgeons, Chicago, IL, September 2012
Evaluation: Students are evaluated as either pass or fail. The instructor
veries the accuracy of the student’s ability to insert an NPA on an airway
trainer by means of observing the student’s procedures and technique.

10
CENTER FOR ARMY LESSONS LEARNED
Materials:
• •
Student checklist
• •
Airway simulator
• •
NPA
• •
Surgical lubricant
Instructor guidelines:
• •
Provide each instructor with a student checklist.
• •
Ensure the student has all student-required materials.
• •
Read the learning objective and the evaluation method to the student.
• •
Explain the grading of the exercise.
• •
Allow students time to extract the information required from the
instructor-provided scenario.
Performance steps:
• •
Assemble and test on all necessary equipment.
• •
Assess the upper airway for visible obstruction.
• •
Open the airway with a chin lift/jaw thrust maneuver.
• •
Verbalize the indications for an NPA (unconscious patient).
• •
Lubricate the NPA with a surgical lubricant.
• •
Insert the airway into the nose at a 90-degree angle to the face. Avoid
aiming upwards toward the top of the head. Insert the airway all the
way to the ange.
• •
Use a rotary and/or back-and-forth motion to facilitate insertion.
• •
If unable to insert on one side of the nasal passage, take it out and try
the other side.

11
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Table 1-1. NPA Evaluation
Task Evaluation
Completed
1st 2nd 3rd
Assessed the upper airway for visible obstruction. pass/
fail
pass/
fail
pass/
fail
Opened the airway with a chin lift/jaw thrust
maneuver.
pass/
fail
pass/
fail
pass/
fail
Lubricated the NPA with a surgical lubricant. pass/
fail
pass/
fail
pass/
fail
Inserted the airway into the nose at a 90-degree
angle to the face. Avoided aiming upwards toward
the top of the head. Inserted all the way to the ange.
pass/
fail
pass/
fail
pass/
fail
Used a rotary and/or back-and-forth motion to
facilitate insertion.
pass/
fail
pass/
fail
pass/
fail
If unable to insert on one side of the nasal passage,
took the NPA out and inserted it on the other side.
pass/
fail
pass/
fail
pass/
fail
Critical criteria:
• •
Aimed the NPA toward the top of the head during insertion.
• •
Performed the procedure in a manner that was dangerous to the
casualty.
Surgical Cricothyroidotomy
Necessary equipment: Prefabricated cricothyroidotomy kit. In the event kits
are unavailable, an improvised kit should include a cutting instrument (for
example, scalpel No. 10 or 15), forceps or tracheal hook, povidone-iodine,
endotracheal tube (ETT), 6 millimeter (mm) gloves, 4- by 4-inch gauze,
tape, local anesthetic, and materials to inject.
NOTE: Cricothyroidotomy sets should be prepared prior to the mission. All
essential pieces of equipment should be prepared before deployment and
packed into a Ziploc bag. Cut the ETT to just above the cuff ination tube
so that the ETT is not protruding 6 inches out of the casualty’s neck.

12
CENTER FOR ARMY LESSONS LEARNED
Figure 1-10. Surgical cricothyroidotomy
1. Hyperextend the casualty’s neck.
• •
Place the casualty in the supine position.
• •
Place a rolled blanket or poncho under the casualty’s neck or between
the shoulder blades so that the airway is straight.
Warning: Do not hyperextend the casualty’s neck if a cervical injury is
suspected.
2. Put on medical gloves, available in the patient’s individual rst aid kit.
3. Locate the cricothyroid membrane.
• •
Place a nger of the nondominant hand on the thyroid cartilage
(Adam’s apple), and slide the nger down to the cricoid cartilage.
• •
Palpate for the “V” notch of the thyroid cartilage.
• •
Slide the index nger down into the depression between the thyroid
and cricoid cartilage.
Figure 1-11. Cricothyroid membrane anatomy

13
TACTICAL COMBAT CASUALTY CARE HANDBOOK
4. Prepare the incision site:
• •
Administer local anesthesia to the incision site if the casualty is
conscious.
• •
Prepare the skin over the membrane with an alcohol pad or povidone-
iodine.
5. With a cutting instrument in the dominant hand, make a 1.5-inch vertical
incision through the skin over the cricothyroid membrane.
Caution: Do not cut the cricothyroid membrane with this incision.
Also, ensure not to perform a horizontal incision.
6. Relocate the cricothyroid membrane by touch and sight.
7. Stabilize the larynx with one hand and make a 1/2-inch transverse
incision through the elastic tissue of the cricothyroid membrane.
NOTE: A rush of air may be felt through the opening.
8. Dilate the opening with a hemostat or scalpel handle. Hook the
cricothyroid membrane with a prefabricated cricothyroid hook or bent
18-gauge needle.
9. Grasp and stabilize the cricoid cartilage.
10. Insert the ETT through the opening and toward the lungs. Only advance
the ETT 2 to 3 inches into the trachea to prevent right main stem bronchus
intubation. Inate the cuff to prevent aspiration.
11. Secure the tube circumferentially around the patient’s neck to prevent
accidental extubation. This can be achieved with tape, tubing, or a
prefabricated device in some kits.
12. Check for air exchange and tube placement:
• •
Air exchange: Listen and feel for air passage through the tube; look for
fogging in the tube.
• •
Tube placement: Bilateral chest sounds/rise and fall of the chest
conrm proper tube placement.
• •
Unilateral breath sounds/rise and fall of the chest indicate a right
main stem bronchus intubation. Withdraw the ETT 1 to 2 inches and
reconrm placement. Ensure not to completely remove the ETT from
the casualty’s trachea.

14
CENTER FOR ARMY LESSONS LEARNED
• •
Air from the casualty’s mouth indicates the tube is directed toward the
mouth. Remove the tube, reinsert, and recheck for air exchange and
placement.
• •
Any other problem indicates the tube is not placed correctly. Remove
the tube, reinsert, and recheck for air exchange.
13. Once the tube is correctly placed, begin rescue breathing, if necessary
and tactically appropriate:
• •
Connect the tube to a bag valve mask and ventilate the casualty at the
rate of 20 breaths per minute.
• •
If a bag valve mask is not available, begin mouth-to-tube resuscitation
at 20 breaths per minute.
14. If the patient is breathing spontaneously, ensure the tube is not
obstructed and continually assess the need for assisted breathing.
15. Apply a sterile dressing. Use either of the following methods:
• •
Make a V-shaped fold in a 4- by 4-inch gauze pad and place it under
the edge of the ETT to prevent irritation to the casualty. Tape securely.
• •
Cut two 4- by 4-inch gauze pads half way through and place on
opposite sides of the tube. Tape securely.
Emergency Surgical Airway Using the Cric-Key Training Skill Sheet
Objective: Demonstrate the procedure for a surgical airway
(cricothyroidotomy) using the Cric-Key.
Reference: No. 0102PP03A Tactical Combat Casualty Care-Military
Personnel Tactical Field Care No. 1, PowerPoint Presentation from Tactical
Combat Casualty Care-Military Personnel Curriculum Update No. 150603.
Evaluation: Students will be evaluated as either pass or fail. The instructor
will verify the accuracy of the student’s ability to perform an emergency
surgical cricothyroidotomy using the Cric-Key on an airway trainer by
means of observing the student’s procedures and technique.
Materials:
• •
Student checklist
• •
Surgical cricothyroidotomy simulator
• •
Betadine/alcohol prep pads
• •
No. 10 or No. 15 scalpel

15
TACTICAL COMBAT CASUALTY CARE HANDBOOK
• •
Cric-Key
• •
5.0 cuffed Melker cricothyroidotomy airway cannula
• •
10 cubic centimeter (cc) syringe
• •
Gauze pads (4 by 4 inches)
• •
Circumferential tie
• •
Ambu bag
Instructor guidelines:
• •
Provide each instructor with a student checklist.
• •
Ensure the student has all student-required materials.
• •
Read the learning objectives and the evaluation method to the student.
• •
Explain the grading of the exercise.
Performance steps:
• •
Assemble and test all necessary equipment.
• •
Verbalize that body substance isolation precautions were considered.
• •
Assess the upper airway for visible obstruction.
• •
Identify the cricothyroid membrane between the thyroid and cricoid
cartilages. On a buddy, identify to the instructor the location of the
top of the thyroid cartilage, the thyroid prominence (on males), the
bottom of the thyroid cartilage, the top of the cricoid cartilage, and the
cricothyroid membrane.
• •
Identify the site of the skin incision. On a buddy, draw a dotted mid-
line from the bottom of the thyroid cartilage to the top of the cricoid
cartilage that overlies and bisects the cricothyroid membrane where
the skin incision would be made for an actual cricothyrotomy.
• •
Palpate the cricothyroid membrane and (while stabilizing the cartilage)
make a vertical incision through the skin (simulate for training)
directly over the cricothyroid membrane.
• •
While continuing to stabilize the larynx, use the scalpel to dissect the
tissues to expose the cricothyroid membrane.
• •
While continuing to stabilize the larynx, use the scalpel to make a
horizontal incision through the cricothyroid membrane.

16
CENTER FOR ARMY LESSONS LEARNED
• •
Insert the Cric-Key with the Melker airway cannula into the trachea,
directed towards the lungs, until the ange contacts the skin of the
neck. Verbalize feeling the tracheal rings with the tip of the Cric-Key
during the insertion.
• •
Remove the Cric-Key, leaving the Melker cannula in place.
• •
Inate the cuff with 10 milliliters (ml) of air.
• •
Check for air exchange and verify placement of the Melker cannula
by listening and feeling for air passing in and out of the tube, causing
the tube to mist. Look for a bilateral rise and fall of the chest. If the
casualty does not breathe spontaneously, connect the Ambu bag to the
cuff of the Melker cannula and ventilate. Check for breathing sounds
bilaterally.
• •
If the position is correct, secure the tube with cotton tape.
• •
Apply a dressing to further protect the tube and incision site.
• •
Monitor the casualty’s respirations. Ventilate if required.
Table 1-2. Emergency surgical airway (cricothyroidotomy) using the
Cric-Key evaluation
Task Evaluation
Completed
1st 2nd 3rd
Assessed the upper airway for visible obstruction. pass/
fail
pass/
fail
pass/
fail
Correctly identied key surface landmarks on the
anterior neck and the cricothyroid membrane on a
buddy.
pass/
fail
pass/
fail
pass/
fail
Correctly marked the site for the skin incision over
the cricothyroid membrane on a buddy.
pass/
fail
pass/
fail
pass/
fail
Palpated the cricothyroid membrane and, while
stabilizing the cartilage, made a vertical incision
through the skin directly over the cricothyroid
membrane.
pass/
fail
pass/
fail
pass/
fail

17
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Table 1-2. Emergency surgical airway (cricothyroidotomy) using the
Cric-Key evaluation (continued)
Task Evaluation
Completed
1st 2nd 3rd
While continuing to stabilize the larynx, used
the scalpel to dissect the tissues to expose the
cricothyroid membrane.
pass/
fail
pass/
fail
pass/
fail
Used the scalpel to make a horizontal incision
through the cricothyroid membrane.
pass/
fail
pass/
fail
pass/
fail
Inserted the Cric-Key and Melker cannula through
the cricothyroid membrane directed distally toward
the lungs until the ange contacted the skin of the
neck.
pass/
fail
pass/
fail
pass/
fail
Verbalized feeling for tracheal rings while inserting
the Cric-Key and Melker cannula.
pass/
fail
pass/
fail
pass/
fail
Removed the Cric-Key, leaving the Melker cannula
in place.
pass/
fail
pass/
fail
pass/
fail
Inated the cuff of the Melker cannula with 10 ml
of air.
pass/
fail
pass/
fail
pass/
fail
If the air exchange was adequate, secured the Melker
cannula in place.
pass/
fail
pass/
fail
pass/
fail
Applied a dressing to further protect the tube and
incision site.
pass/
fail
pass/
fail
pass/
fail
Monitored the casualty's respirations. pass/
fail
pass/
fail
pass/
fail

18
CENTER FOR ARMY LESSONS LEARNED
Critical criteria:
• •
Did not obtain a patent airway with the emergency surgical airway.
• •
Did not correctly identify the location of the cricothyroid membrane.
• •
Performed the procedure in a manner that was dangerous to the
casualty.
King Laryngeal Tube (LT) Insertion
Necessary equipment: King LT, water-based lubricant, and a syringe.
1. Prepare the casualty:
• •
Place the casualty’s head in the “snifng” position.
• •
Preoxygenate the casualty, if equipment is available.
2. Prepare the King LT:
• •
Choose the appropriately sized tube.
• •
Test cuff ination by injecting the proper volume of air into the cuff.
Deate the cuff prior to inserting the tube.
• •
Lubricate the tube with a water-based lubricant.
Caution: Do not use a petroleum-based or non-water-based lubricant.
These substances can cause damage to the tissues lining the nasal
cavity and pharynx, increasing the risk for infection.
3. Insert the King LT.
• •
Hold the tube in the dominant hand. With the nondominant hand, open
the casualty’s mouth, and apply a chin lift.
• •
With the King LT rotated laterally 45 to 90 degrees, place the tip into
the mouth and advance the tube behind the base of the tongue.
NOTE: A lateral approach with the chin lift facilitates proper insertion. The
tip must remain midline as it enters the posterior pharynx.
• •
Rotate the tube to midline as the tip reaches the posterior pharynx.
• •
Advance the tube until the base of the connector is aligned with the
teeth or gums.
• •
Using either an attached pressure gauge or syringe, inate the cuff to
the minimum volume necessary to seal the airway.

19
TACTICAL COMBAT CASUALTY CARE HANDBOOK
4. Conrm proper placement of the tube.
• •
Reference marks for the tube are at the proximal end of the tube and
should be aligned with the upper teeth.
• •
Conrm proper placement by listening for equal breath sounds during
ventilation.
• •
While gently ventilating the casualty, withdraw the tube until
ventilation is easy and free owing, with minimal airway pressure
needed.
NOTE: Initially placing the tube deeper than required and then withdrawing
slightly increases the chance of proper insertion, helps ensure a patent
airway, and decreases the risk of airway obstruction if the casualty
spontaneously ventilates.
5. Secure the tube with tape.
Breathing Management
(Addressed During Tactical Field Care and Tactical Evacuation Care Phases.
See Chapter 2, Tactical Combat Casualty Care Phases of Care, Pages 45 and 46.)
Penetrating Chest Wounds
Necessary equipment: Prefabricated chest seal or any airtight material
(plastic wrap).
1. Expose the wound(s):
• •
Cut or unfasten the clothing that covers the wound and expose
the casualty’s torso from the umbilicus to the Adam’s apple
circumferentially.
• •
Wipe blood/sweat from skin surrounding the wound to increase the
occlusive seal’s effectiveness.
• •
Disrupt the wound as little as possible.
• •
Apply an occlusive seal to any penetrating injuries on the torso.
NOTE: Do not remove clothing stuck to the wound.
2. Check for an exit wound.
• •
Logroll the casualty and look at the back.
• •
Remove the casualty’s clothing, if necessary.

20
CENTER FOR ARMY LESSONS LEARNED
3. Seal the wound(s), treating each wound as you go. When not using a
prefabricated chest seal, cut the dressing’s plastic wrapper on one long and
two short sides and remove the dressing.
• •
Apply the inner surface of the wrapper to the wound when the casualty
exhales.
• •
Ensure that the covering extends at least 2 inches beyond the edges of
the wound.
• •
Seal by applying overlapping strips of tape to all edges of occlusive
dressing, forming a complete seal.
• •
Cover all wounds in the same manner, as applicable.
NOTE: All penetrating chest wounds should be treated as if they are
penetrating chest wounds.
NOTE: In an emergency, any airtight material can be used. The material
must be large and durable enough so it is not sucked into the chest cavity.
4. Place the casualty on the injured side or sitting up.
5. Monitor the casualty for increasing respiratory difculty:
• •
Monitor breathing and the wound seal for continued effectiveness.
• •
Check vital signs.
• •
Observe for signs of shock.
Needle Chest Decompression
Necessary equipment: Large-bore needle with catheter (10- to 14-gauge, at
least 3.25 inches in length) and tape.
1. Locate the second intercostal space (between the second and third ribs) at
the midclavicular line (approximately in line with the nipple) on the affected
side of the casualty’s chest (see Figure 1-12). (An acceptable alternative site
is located at the fourth or fth rib space at the anterior axillary line [refer to
Figure 1-13]).
2. Insert a large-bore (10- to 14-gauge) needle/catheter unit.
• •
Place the needle tip on the insertion site (between the second and third
intercostal space, midclavicular line).
• •
Lower the proximal end of the needle to permit the tip to enter the skin
just above the third rib margin.

21
TACTICAL COMBAT CASUALTY CARE HANDBOOK
• •
Firmly insert the needle into the skin over the third rib at a 90-degree
angle to the chest wall until the pleura has been penetrated, as
evidenced by feeling a “pop” as the needle enters the pleural space and
a hiss of air escapes from the chest.
Warning: Proper positioning of the needle is essential to avoid
puncturing blood vessels and/or nerves. The needle should not be
inserted medial to the nipple line, as this will increase the risk of the
needle entering the cardiac box.
NOTE: If you are using a catheter-over-needle, the catheter should be
inserted to the hub. Withdraw the needle along the angle of insertion while
holding the catheter still.
3. Secure the catheter to the chest with tape and monitor the casualty for
possible return of symptoms.
NOTE: Do not occlude the end of the catheter with the tape. Air needs to
ow freely through the catheter.
4. Monitor the patient for signs and symptoms of a recurring tension
pneumothorax:
• •
If a tension pneumothorax returns, reassess all interventions (chest
seals and needle chest decompressions).
• •
If a chest seal becomes dislodged, replace it.
• •
If a needle chest decompression catheter has become occluded, insert
a second catheter in accordance with step 2 of the instructions directly
laterally of the rst catheter on the mid-clavicular line (primary site)
or directly superior of the rst catheter on the anterior axillary line
(alternate site).
Figure 1-12. Needle chest compression,
needle insertion site

22
CENTER FOR ARMY LESSONS LEARNED
Chest Tube Insertion
Necessary equipment: Chest tube (catheter 16 to 35 Fr), gloves, one-
way valve, scalpel handle with blades (No. 10 or No. 15), Kelly forceps,
large hemostat, povidone-iodine, suture material, lidocaine with 1 percent
epinephrine for injection, needle, and syringe.
1. Assess the casualty:
• •
If necessary, open the airway.
• •
Ensure adequate respiration and assist as necessary.
• •
Provide supplemental oxygen, if available.
• •
Connect the casualty to a pulse oximeter, if available.
2. Prepare the casualty.
• •
Place the casualty in the supine position.
• •
Raise the arm on the affected side above the casualty’s head.
• •
Select the insertion site at the anterior axillary line over the fourth or
fth intercostal space.
• •
Clean the site with povidone-iodine solution.
• •
Put on sterile gloves.
• •
Drape the area.
• •
Liberally inltrate the area with the 1 or 2 percent lidocaine solution
and allow time for medication to take effect if patient symptoms
permit.
3. Insert the tube:
• •
Make a 2 to 3 centimeter (cm) transverse incision over the selected site
and extend it down to the intercostal muscles.
NOTE: The skin incision should be 1 to 2 cm below the intercostal space
through which the tube will be placed.
• •
Insert the large forceps through the intercostal muscles in the next
intercostal space above the skin incision.
• •
Puncture the parietal pleura with the tip of the forceps and slightly
enlarge the hole by opening the clamp 1.5 to 2 cm.

23
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Caution: Avoid puncturing the lung. Always use the superior margin of
the rib to avoid the intercostal nerves and vessels.
• •
Immediately insert a gloved nger in the incision to clear any
adhesions, clots, etc.
• •
Grasp the tip of the chest tube with forceps. Insert the tip of the tube
into the incision as you withdraw your nger.
• •
Advance the tube until the last side hole is 2.5 to 5 cm inside the chest
wall.
• •
Connect the end of the tube to a one-way drainage valve (e.g.,
Heimlich valve or improvised).
• •
Secure the tube using the suture materials.
• •
Apply an occlusive dressing over the incision site.
• •
Radiograph the chest to conrm placement, if available.
4. Reassess the casualty.
• •
Check for bilateral breath sounds.
• •
Monitor and record vital signs every 15 minutes.
5. Document the procedure.
Figure 1-13. Chest tube insertion site

24
CENTER FOR ARMY LESSONS LEARNED
Vascular Access
(Addressed During Tactical Field Care and Tactical Evacuation Care Phases.
See Chapter 2, Tactical Combat Casualty Care Phases of Care, Pages 45 and 46.)
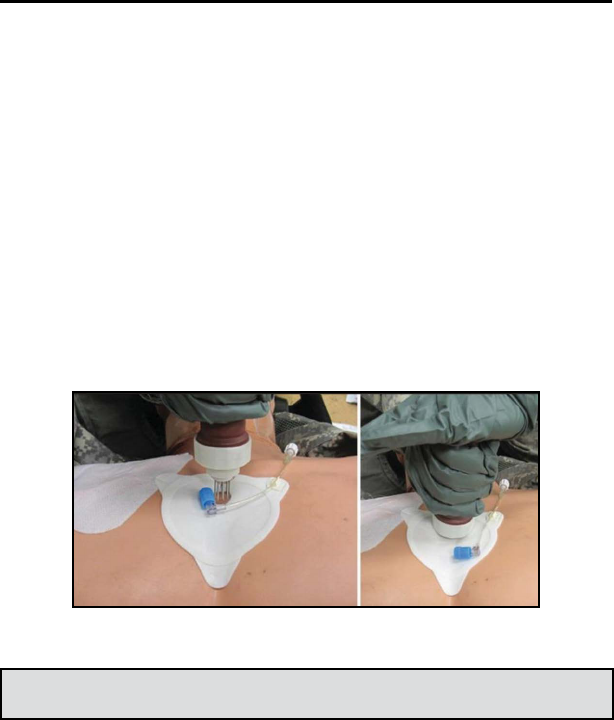
Intraosseous Placement: First Access for Shock and Trauma (FAST1)
System
Necessary equipment: FAST1 System device, 10 cc syringe with normal
saline for ush, saline lock, and tape.
1. Positioning and preparing the site:
• •
Providers should position themselves above the head of the casualty to
avoid improper insertion of the device.
• •
Expose the sternum.
• •
Identify the sternal notch (not the xyphoid process).
2. Place the target patch.
• •
Remove the top half of the backing (“Remove 1”) from the patch.
• •
Place the index nger on the sternal notch, perpendicular to the skin.
• •
Align the locating notch in the target patch with the sternal notch.
• •
Verify that the target zone (circular hole) of the patch is directly over
the casualty’s midline, and press rmly on the patch to engage the
adhesive and secure the patch.
• •
Remove the remaining backing (“Remove 2”) and secure the patch to
the casualty.
Figure 1-14. FAST1 target patch
25
TACTICAL COMBAT CASUALTY CARE HANDBOOK
3. Insert the introducer:
• •
Position yourself over the head of the patient facing toward the
patient’s feet.
• •
Remove the cap from the introducer.
• •
Place the bone probe cluster needles in the target zone of the target
patch.
• •
Hold the introducer perpendicular to the skin of the casualty.
• •
Pressing straight along the introducer axis, with hand and elbow in
line, push with a rm, constant force until a release is heard and felt.
• •
Expose the infusion tube by gently withdrawing the introducer. The
stylet supports will fall away.
Figure 1-15. FAST1 introducer insertion
Warning: Avoid extreme force or twisting motions.
4. Connect the infusion tube.
• •
Connect the infusion tube to the right-angle female connector (blue
tip).
• •
Flush the catheter with 10 ml of sterile IV solution.
• •
Also may add 2 to 3 ml of 2 percent lidocaine to reduce pain during
the infusion.
• •
Attach a saline lock to the remaining Luer lock connector.

26
CENTER FOR ARMY LESSONS LEARNED
Figure 1-16. Secure with protector dome
5. Place the protector dome directly over the target patch and press rmly to
engage the Velcro fastening.
6. Reinforce with tape.
FASTResponder
Precautions:
• •
The FASTResponder is designed to penetrate 6 mm into the
manubrium. Qualied professionals should determine any appropriate
or necessary exceptions, either inclusions or exclusions, to the
criterion for patients 12 years and older.
• •
The proximal tip of the infusion tube contains metal.
• •
The function of the device may be affected by:
Compromised skin over the insertion site such as trauma,
infection, or burns
Fracture of the sternum or vascular injury, which may compromise
the integrity of the manubrium or its vascularization
Midline sternotomy scars

27
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Figure 1-17. FASTResponder device
Warnings:
• •
Safety in patients with very severe osteoporosis has not been proven.
• •
Insertion in sites other than the manubrium may result in ineffective
infusion and/or serious injury to the patient.
• •
Reuse of FASTResponder is not recommended due to the potential of
cross-contamination, which may lead to serious injury or death. The
FASTResponder is unlikely to function after use.
• •
Do not insert nger(s) in the open end of the device due to the
potential of a needle stick.

28
CENTER FOR ARMY LESSONS LEARNED
1. Expose the sternum and clean the infusion site.
NOTE: Maintain aseptic technique throughout the procedure.
NOTE: Administer local anesthetic if the patient is conscious and alert.
Figure 1-18
2. Remove the adhesive liner with the locking pin.
Figure 1-19
3. Align the target foot notch with the patient’s sternal notch, over the
midline, and perpendicular to the manubrium.
Figure 1-20

29
TACTICAL COMBAT CASUALTY CARE HANDBOOK
4. Push the FASTResponder down completely to deploy the infusion tube.
Figure 1-21
5. Withdraw the FASTResponder straight back while holding down the
target foot. The support comes out with the infusion tube. Discard the
FASTResponder following local contaminated sharps protocols.
Figure 1-22

30
CENTER FOR ARMY LESSONS LEARNED
6. Connect the IV line directly to the Luer, and clip the strain relief hook to
the target foot. Optional: Conrm placement by aspiration, and ush with
uid to clear.
Figure 1-23
7. Optional: Remove the liner from the protective dome and apply the dome
over the target foot infusion site.
Figure 1-24

31
TACTICAL COMBAT CASUALTY CARE HANDBOOK
8. FASTResponder removal:
• •
Turn off the source of uid and disconnect. Pull on the infusion tube
to remove it from the patient. Peel off the target foot and dress the site
per standard protocol.
• •
Discard the infusion tube and target foot following local contaminated
sharps protocols.
NOTE: Removal should only be performed by a physician or nurse.
NOTE: Pull the infusion tube using one continuous motion (do not start/
stop) until removal. Pull on the tube, not the Luer connection. It is normal
for the tubing to stretch.
Figure 1-25

32
CENTER FOR ARMY LESSONS LEARNED
Intraosseous Access with the Sternal EZ-IO Needle Set
The Sternal EZ-IO is used to obtain IO vascular access in adults in whom
rapid uid resuscitation or pharmacological treatment is needed emergently,
and standard IV access is not readily accessible.
The sternal EZ-IO needle/driver set is green, and comes in green packaging.
It is designed for insertion into the manubrium of the sternum, and should
not be used for IO access at any other site. Conversely, the manual EZ-
IO needle/driver intended for use on the humerus or tibia is blue, and this
needle should never be used on the sternum. The sternal needle also has a
depth-limiting “collar” on the catheter, which is not present on the catheter
of the limb device.
Figure 1-26
If the manubrium is fractured, IO access through it should not be attempted.
Fluid follows the path of least resistance. If an IO device is placed in a
fractured bone, the uid would simply extravasate into the surrounding
tissue through the fracture site.
Contraindications consist of:
• •
Fracture of the manubrium
• •
Previous surgical procedure
• •
Manubrial IO within the past 24 to 48 hours
• •
Infection at the insertion site
• •
Inability to locate landmarks or excessive tissue over the target site

33
TACTICAL COMBAT CASUALTY CARE HANDBOOK
1. With proper insertion, the needle tip should lie in the marrow cavity of
the manubrium.
Figure 1-27
2. Expose the chest and identify the insertion site by palpation. The sternal
insertion site is located midline, approximately 1 to 2 cm below the sternal
notch. Once the insertion site is identied, clean the area with alcohol or
povidone-iodine.
Figure 1-28

34
CENTER FOR ARMY LESSONS LEARNED
3. Remove tab 1 from the sternal locator. Align the curve at the top of the
sternal locator with the suprasternal notch, and adhere the top half of the
sternal locator to the patient. Holding the sternal locator in place, pull
tab 2 to expose the adhesive on the bottom half of the sternal locator. Press
the sternal locator down on the chest to ensure it adheres to the casualty’s
skin.
Figure 1-29
4. Carefully nick the skin over the insertion site with the provided lancet
through the sternal locator. The length of the nick should not exceed 3 mm,
which is the width of the nger lancet and the opening in the sternal locator.
NOTE: It is imperative that the nick reaches all the way down to the sternal
bone at the insertion site. Failure to do so could lead to improper or failed
placement.

35
TACTICAL COMBAT CASUALTY CARE HANDBOOK
5. Keep the casualty still while inserting the needle. Position the sternal
needle set at the insertion site with the needle perpendicular to the plane
of the manubrium. Gently insert the needle set into the incision until the
needle touches bone. Penetrate the bone cortex by rotating clockwise
and counterclockwise while applying gentle, steady, downward pressure.
Stop insertion when a sudden lack of resistance is felt upon entry into
the medullary space. Do not rock or bend the needle set while it is being
inserted. Maintain the 90-degree angle.
NOTE: Use gentle, steady pressure, not excessive force. Allow the catheter
tip rotation and gentle downward pressure to provide the penetrating action.
Figure 1-30
6. Remove the stylet:
• •
Manually stabilize the hub.
• •
Rotate the stylet counterclockwise, then pull it out.
Figure 1-31

36
CENTER FOR ARMY LESSONS LEARNED
7. Apply the stabilizer to the catheter hub without removing the sternal
locator. Once the stabilizer is in position, prime the EZ-Connect Extension
Set with normal saline, attach it to the catheter hub and tighten it rmly.
Tightening of the EZ-Connect sets the catheter/stabilizer height into a xed
position. To secure the stabilizer, hold the catheter still while pulling away
each of the numbered tabs.
Figure 1-32
8. A rmly seated catheter, the ability to administer pressurized uids
without difculty, and noting the pharmacologic effects of any uids or
medications given are indicators of successful cannulation of the medullary
space.
Conrm catheter placement:
• •
Firmly seated catheter
• •
Flash of blood or blood on aspiration (may or may not be able to
aspirate blood)
• •
Pressurized uids ow freely
• •
Pharmacologic effects
Conrmation of catheter placement can be achieved by aspiration. Attach
a syringe to the primed extension set, and slowly retract the plunger to
withdraw marrow. If marrow is present, the needle has been successfully
placed in the medullary space. Blood may also be noted in the hub of
the needle when you remove the stylet. Absence of blood or inability to
withdraw aspirate at the catheter hub does not mean the insertion was
unsuccessful.

37
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Figure 1-33
9. Once the catheter placement has been conrmed, the site should be
continually re-evaluated for signs of extravasation, uid leakage, or any
other signs that indicate the needle tip is no longer in the medullary space.
Flush the catheter:
• •
Connect the syringe to primed extension set
• •
Flush with 10 ml normal saline
• •
Multiple ushes may be needed
• •
No ush equals no ow
10. The intraosseous space is occupied by bone marrow held in place by a
thick brin network. In order to obtain maximum ow rates, this brin mesh
must be displaced. This is achieved with a rapid 10 ml ush with normal
saline. The initial ush will be met with inherent resistance as the brin
mesh is being displaced. After the rst vigorous ush of normal saline, uid
ow through the IO device should be easy and rapid. Occasionally, more
than one ush may be required to obtain maximum ow rates.
NOTE: No ush, no ow. If this step is omitted, optimal ow rates will not
be achieved.
Figure 1-34

38
CENTER FOR ARMY LESSONS LEARNED
11. Infuse uids with pressure:
• •
The pressure in the medullary space is about one-third of the casualty’s
arterial pressure.
• •
Pressurizing uids for infusion is required to achieve maximum ow
rates.
Figure 1-35
12. Sternal EZ-IO removal:
• •
Remove the EZ-Connect extension set and stabilizer.
• •
Attach a Luer lock syringe directly to the hub.
• •
Rotate the syringe clockwise while slowly and gently pulling straight
back.
• •
Maintain axial alignment. Do not rock the syringe.
• •
Remove the sternal locator.

39
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Peripheral Intravascular Access
Necessary equipment: IV tubing, IV uids, 18-gauge or larger IV needle
with catheter, saline lock, constricting band, antiseptic wipes, gloves, tape,
and 2- by 2-inch gauze sponges.
1. Put on gloves.
2. Select an appropriate access site on an extremity:
• •
Avoid sites over joints.
• •
Avoid injured extremities.
• •
Avoid extremities with signicant wounds proximal to the IV insertion
site.
3. Prepare the site:
• •
Apply the constriction band around the limb, about 2 inches above the
puncture site.
• •
Clean the site with antiseptic solution.
5. Puncture the vein:
• •
Stabilize the skin at the puncture site with the nondominant thumb,
pulling the skin downward until taut. Avoid placing the thumb directly
over the vein to avoid collapsing.
• •
Position the needle point, bevel up, parallel to the vein, 1/2 inch below
the venipuncture site.
• •
Hold the needle at a 20- to 30-degree angle and insert it through the
skin.
• •
Move the needle forward about 1/2 inch into the vein.
• •
Conrm the puncture by observing blood in the ash chamber.
NOTE: A faint give may be felt as the needle enters the vein.
6. Advance the catheter.
• •
Grasp the hub and advance the needle into the vein up to the hub.
(NOTE: This prevents back ow of blood from the hub.)
• •
While holding the hub, press lightly on the skin with the ngers of the
other hand.

40
CENTER FOR ARMY LESSONS LEARNED
• •
Remove the needle from the catheter and secure it in a safe place to
avoid accidental needle sticks.
• •
Attach a saline lock, preferably needleless.
7. Connect the catheter to the IV infusion tubing. An 18-gauge needle will
be required, if not using a needleless saline lock.
• •
Begin the infusion.
• •
Observe the site for inltration of uids into the surrounding soft
tissue.
8. Secure the catheter and tubing to the skin and dress the site.
Hypothermia Prevention
(Addressed During Tactical Field Care and Tactical Evacuation Care Phases.
See Chapter 2, Tactical Combat Casualty Care Phases of Care, Pages 45 and 46.)
1. Stop bleeding and resuscitate appropriately. Use warm uids, if available.
2. Remove any wet clothes and replace with dry clothes, if possible.
3. Use the Hypothermia Prevention and Management Kit (HPMK).
• •
Place the casualty on a Blizzard Survival Blanket or heat-reective
shell to maintain body temperature.
• •
Place a Ready-Heat blanket on the casualty’s torso to aid in increasing
body temperature. Do not place the Ready-Heat blanket directly on the
casualty’s skin, which may cause a burn.
• •
Wrap the Blizzard Survival Blanket or heat-reective shell around the
casualty. If a survival blanket of any kind is not available, then nd
dry blankets, poncho liners, space blankets, sleeping bags, body bags,
or anything that will retain heat and keep the casualty dry.

41
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Tactical evacuation care phase:
1. The casualty should remain wrapped in the Blizzard Survival Blanket or
Heat-Reective Shell with Ready-Heat blanket while awaiting evacuation;
en route care should be provided.
2. If these items were not available in the other phases of care, check with
evacuation personnel to see if they have them or any other items that can be
used to prevent heat loss.
3. Wrap the casualty in dry blankets and, during helicopter transport, try to
keep the wind from open doors from blowing over or under the casualty.
4. Use a portable uid warmer on all IO/IV sites and for all liquid
medication administered (Hextend, Lactated Ringers, TXA, blood, etc.).
Administering cold uids contributes to the likelihood of the casualty
developing hypothermia.

42
CENTER FOR ARMY LESSONS LEARNED
Tactical Field Care Basic Management Plan
NOTE: Casualties with an altered mental status should be disarmed
immediately.
• •
Massive hemorrhage:
Assess for an unrecognized hemorrhage and control all sources of
bleeding.
Use one or more CoTCCC-recommended limb tourniquets, if
necessary.
Use a CoTCCC-approved hemostatic dressing for compressible
hemorrhage not amenable to limb tourniquet use or as an adjunct
to tourniquet removal.
Immediately apply a CoTCCC-recommended junctional
tourniquet if the bleeding site is amenable to use of a junctional
tourniquet.
Reassess the prior tourniquet application:
•••*
Expose the wound and determine if a tourniquet is needed.
•••*
Replace any limb tourniquet placed over the uniform with
one applied directly to the skin, 2 to 3 inches above the
wound.
Expose and use an indelible marker to clearly mark all tourniquet
sites with the time of tourniquet application.
• •
Airway management:
Conduct the following for an unconscious casualty without an
airway obstruction:
•••*
Chin lift/jaw thrust maneuver.
•••*
NPA.
•••*
Place the casualty in the recovery position (see Figure 1-38).
Figure 1-38. Recovery position

43
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Conduct the following for a casualty with an airway obstruction or
impending airway obstruction:
•••*
Chin lift/jaw thrust maneuver.
•••*
NPA.
•••*
Allow a conscious casualty to assume any position that best
protects the airway to include sitting up.
•••*
Place an unconscious casualty in the recovery position.
•••*
If these measures are unsuccessful, refer to a medic
immediately. Perform a surgical cricothyroidotomy using
one of the following:
•••••♦
CricKey technique.
•••••♦
Bougie-aided open surgical technique.
•••••♦
Standard open surgical technique.
•••••♦
Lidocaine, if the casualty is conscious.
• •
Respirations:
For a casualty with progressive respiratory distress and known or
suspected torso trauma, consider a tension pneumothorax.
All open and/or sucking chest wounds should be treated by:
•••*
Immediately applying a vented chest seal to cover the defect.
•••*
If a vented chest seal is not available, use a non-vented chest
seal.
•••*
Burping or temporarily removing the dressing. If this does
not relieve the respiratory distress, refer to a medic.
• •
Circulation:
Assess the casualty for hemorrhagic shock. If the casualty is not in
shock, oral uids are permissible if the casualty is conscious and
can swallow.
If the casualty is in shock, refer to a medic.

44
CENTER FOR ARMY LESSONS LEARNED
• •
Hypothermia prevention:
Minimize casualty environmental exposure and promote heat
retention.
Keep personal protective gear on, if feasible. Replace wet
clothing, if possible. Get the casualty onto an insulated surface as
soon as possible.
Use CoTCCC-approved hypothermia prevention kit, if available.
If a hypothermia prevention kit is not available, then use dry
blankets, poncho liners, sleeping bags, or anything that will retain
heat and keep the casualty warm and dry.
• •
Pain management:
Analgesia on the battleeld should generally be achieved by one
of following options:
•••*
If there is mild to moderate pain and/or the casualty is able
to ght, give the casualty a TCCC combat wound pill pack
(CWPP).
•••*
If there is moderate to severe pain and the casualty is not in
shock, refer to a medic.
• •
Antibiotics (recommended for all open combat wounds):
If the casualty can swallow, administer 400 mg of moxioxacin
from the CWPP.
If the casualty cannot swallow (shock or unconsciousness), refer
to a medic.
• •
Wounds:
Inspect and dress known wounds.
Check for additional wounds (for example, scalp lacerations).
• •
Splinting:
If a penetrating eye injury is noted or suspected, conduct the
following:
•••*
Cover the eye with a rigid eye shield and not a pressure
patch.
•••*
Administer 400 mg moxioxacin from the CWPP.
Splint fractures.

45
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Chapter 2
Tactical Combat Casualty Care Phases of Care
Understanding phases of care is important for proper application of Tactical
Combat Casualty Care (TCCC) principles. Properly balancing winning the
ght, accomplishing the mission, and treating casualties is essential for
success tactically as well as medically. This chapter discusses the proper
tactics and medicine for each phase of care.
Phase 1: Care Under Fire (CUF)— Return Fire
Figure 2-1. Phase 1: CUF
• •
Good tactics: CUF is conducted while tactically engaged. The
most effective way to reduce morbidity and mortality is the precise
application of combat res by all personnel. Continue the tactical
mission, gain re superiority, then treat casualties.
• •
Good medicine: Massive hemorrhage. The control of extremity
hemorrhage with direct pressure while applying a hasty tourniquet is
the primary medical goal during CUF. A tourniquet is the single most
important medical intervention rendered at the point of injury (POI).
Phase 2: Tactical Field Care (TFC)— Move Casualty to
Cover
Figure 2-2. Phase 2: TFC

46
CENTER FOR ARMY LESSONS LEARNED
• •
Good tactics: When no longer receiving effective enemy re, the
TFC phase is entered, allowing more medical intervention. Disarm
the casualty, if the casualty’s mental status is altered or if receiving
ketamine or fentanyl. Medical personnel are responsible for activity
inside the casualty collection point (CCP) and leadership is responsible
for activity outside the CCP. Basic life support (cardiopulmonary
resuscitation [CPR]) is typically not performed in combat.
• •
Good medicine:
Massive hemorrhage. Convert hasty tourniquets to deliberate
tourniquets. Pack wounds with combat gauze. Apply a junctional
tourniquet.
Airway. Check the airway for patency. Apply a nasopharyngeal
airway (NPA) and ventilate with a bag-valve mask (BVM), such
as a Cyclone BVM. If the airway shows resistance or evidence of
facial trauma, perform a cricothyrotomy.
Respirations. Apply a vented chest seal to open entry and
exit chest wounds. Treat a tension pneumothorax (PTX) by
decompressing the chest at the mid-clavicular line at the
second and third intercostal space using a 3.25-inch, 14-gauge
angiocatheter and needle chest decompression (NCD).
Circulation. Resuscitate with hypovolemic uid resuscitation
through intravenous (IV) access. Intraosseous (IO) access is
recommended for rapid uid delivery and resuscitation.
Head injury/hypothermia. Perform a Military Acute Concussion
Evaluation (MACE) exam or the alert, verbal, pain, unresponsive
(AVPU) assessment, and document the ndings. Cover the
casualty in an HPMK, body bag, or sleeping bag for warmth.
Phase 3: Tactical Evacuation Care
Figure 2-3. Phase 3: TEC

47
TACTICAL COMBAT CASUALTY CARE HANDBOOK
• •
Good tactics: Move the casualty. The term tactical evacuation
(TACEVAC), as dened in Joint Publication (JP) 4-02, Health
Service Support, 26 July 2012, is medical evacuation (MEDEVAC)
(MEDEVAC-dedicated vehicle) and casualty evacuation (CASEVAC)
(non-medical vehicle). This phase involves initiating air evacuation
with a 9-Line MEDEVAC request and establishing ground ambulance
exchange points.
• •
Good medicine: Re-evaluate the casualty and all interventions. Afx
a pelvic binder if the injuries are caused by a blast, vehicle rollover,
or building collapse. Document all care provided on Department of
Defense (DD) Form 1380, Tactical Combat Casualty Care (TCCC)
Card, June 2014. The TCCC Card format matches the MIST
(mechanism of injury, injuries, signs/symptoms, and treatment) Report
for each casualty on the 9-Line MEDEVAC request.
Continuum of Care
It is important for TCCC-trained individuals to understand the continuum of
care. Having an understanding of different facilities in the immediate area
can factor into MEDEVAC plans. In accordance with JP 4-02, the following
facilities provide higher medical care once the casualty is tactically
evacuated. These facilities are referred to as roles, not levels or echelons.
Role 1
Figure 2-4. Role 1 facilities
Role 1 care consists of prehospital medical care to include self-aid, buddy
aid, and care provided by a combat medic. The battalion aid station or
unit-level medical care facility is a Role 1 facility and provides medical
treatment supervised by a physician assistant or physician. Role 1 facilities
provide advanced trauma management (damage control resuscitation) and
routine sick call. Documentation is completed using the TCCC Card and
MIST Report.

48
CENTER FOR ARMY LESSONS LEARNED
• •
Advanced trauma management is provided at Role 1 facilities (damage
control resuscitation).
• •
Routine sick call is provided in accordance with the U.S. Army Health
Services Command Pamphlet 40-7-21, Algorithm-Directed Troop
Medical Care (ADTMC), June 1992. ADTMC presents every combat
medic, corpsman, or medical technician an algorithm for common
ailments and for diseases and non-battle injuries (DNBIs).
Role 2
Figure 2-5. Role 2 facilities
In accordance with JP 4-02, a Role 2 facility provides advanced trauma
management and emergency medical treatment, including continuation of
resuscitation started at Role 1 care. Capabilities of a Role 2 facility include
blood products, limited X-ray, limited laboratory, dental support, combat
and operational stress control, preventive medicine, and limited patient hold
for 72 hours.
• •
Role 2 NATO care includes damage control surgery. U.S. Armed
Forces subscribe to the Role 2 medical treatment facility, providing
greater resuscitative capability than what is available at a Role 1
facility. Surgical capability is not mandatory. The Role 2 facility is
the transition point from MARCH (massive hemorrhage, airway,
respirations, circulation, head injury/hypothermia) treatment and the
TCCC Card to the airway, breathing, circulation, disability, exposure
(ABCDE) method and DD Form 3019, Resuscitation Record, October
2015.
• •
Role 2 Army facilities have medical assets located in the treatment
platoons of medical companies and troops, and include basic and
emergency treatment (advanced trauma management). These facilities
have the capability to deliver packed red blood cells (liquid), limited
X-ray, clinical laboratory, dental support, combat and operational
stress control, and preventive medicine.

49
TACTICAL COMBAT CASUALTY CARE HANDBOOK
The medical company brigade support battalion is assigned
to modular brigade combat teams, which include the airborne
brigade combat team (ABCT), infantry brigade combat team
(IBCT), Stryker brigade combat team (SBCT), and the medical
troop in the armored cavalry regiment.
The medical company area support medical battalion provides
direct support to the modular division and support to echelons
above brigade units.
The forward resuscitative and surgical team (FRST) is assigned
to the medical command or medical brigade and attached to the
combat support hospital when not operationally employed forward
with a medical company. The FRST provides damage control
surgery support in the brigade combat team area. This 20-person
team provides a rapidly deployable, immediate damage control
surgery capability utilizing two orthopedic surgeons, two general
surgeons, two nurse anesthetists, two emergency physicians,
and emergency room and critical care nurses and technicians.
The FRST includes two operating tables for a maximum of
10 cases per day and a total of 30 operations. The supporting
medical company must provide logistical support (additional
electricity, water, and fuel); security; and X-ray, laboratory, and
patient administration support. The FRST is designed to be split,
providing maximum exibility to support operations.
• •
Role 2 Air Force
The mobile eld surgical team (MFST) consists of a ve-person
team: general surgeon, orthopedist, anesthetist, emergency
medicine physician, and operating room nurse or technician.
MFST provides 10 lifesaving or limb-saving procedures in 24 to
48 hours from ve backpacks (350-pound total gear), which are
designed to augment a Role I facility.
The small portable expeditionary aeromedical rapid response
(SPEARR) team consists of a 10-person team (includes a ve-
person MFST and three-person critical care air transportation
team), designed to provide surgical support, basic primary care,
postoperative critical care, and preventive medicine for the early
phase of deployment. The SPEARR team is highly mobile, being
able to t all equipment in a one-palletized trailer.

50
CENTER FOR ARMY LESSONS LEARNED
The expeditionary medical support (EMEDS) health response
team (HRT) is the basic EMEDS capability consisting of 40
personnel. The HRT can stabilize and hold four patients for 24
hours. It provides medical and surgical support for an airbase,
providing sick-call, resuscitative surgery, dental care, and limited
laboratory and X-ray capabilities. The 25-member staff includes a
SPEARR team and can provide for 10 operating room cases with
two beds in 24 to 48 hours and four intensive care unit beds and
tents transportable on three pallets.
EMEDS+10 is the second increment of the EMEDS capability
and builds on EMEDS HRT, adding six beds to EMEDS basic.
EMEDS+10 provides medical, surgical, and critical care
augmentation; laboratory service; additional bioenvironmental
engineering; public health; administration; and medical logistics
support with a 56-person staff consisting of six tents transported
on 14 pallets.
• •
Role 2 Navy
A casualty receiving and treatment ship (CRTS) is part of an
amphibious ready group (ARG). An ARG typically comprises
three ships with surgical capability only on the CRTS. Ships have
176 medical personnel supporting 45 ward beds, four operating
rooms (one surgeon, one certied registered nurse anesthetist,
one critical-care nurse, one operating room nurse, one general
medical ofcer, and 12 support staff), and 17 intensive care
unit beds. A CRTS and eet surgical team can be augmented
with 84 additional personnel to increase capability from one
operating room to four. Ships have laboratory, X-ray, frozen blood
capabilities, and triage areas for 50 casualties. Doctrinal holding
capability is limited to three days.
The aircraft carrier battle group includes one operating room,
52 ward beds, and 3 intensive care beds. The staff includes one
surgeon and ve additional medical ofcers. Medical assets
aboard aircraft carriers are intended for use by the aircraft carrier
and its task force. Aircraft carriers are not casualty receiving
ships and are not included in medical assets for support to ground
forces.

51
TACTICAL COMBAT CASUALTY CARE HANDBOOK
A surgical company (SC) provides surgical care for the Marine
Expeditionary Force. The SC provides stabilizing surgical
procedures (damage control surgery) with four forward
resuscitative surgical systems, four shock trauma platoons, and
four en route care teams. An SC has a 20-bed capability for 72
hours, portable digital X-ray, and minimal laboratory and blood-
banking capabilities.
The forward resuscitative surgical system (FRSS) is an 8-person
team (two surgeons, anesthesia, critical care nurse, two operating
room technicians, and two corpsmen). The FRSS provides a high
mobility resuscitative surgery asset for 18 patients within 48 hours
without resupply. The en-route care team is a two-person team
consisting of a critical care registered nurse and a corpsman.
Role 3
Figure 2-6. Role 3 facilities
A Role 3 facility (combat support hospital or EMEDS+25) is a medical
treatment facility or veterinary facility (for working animals) staffed and
equipped to provide care to all categories of patients. Capabilities of a
Role 3 facility include burn management; optometry and ophthalmology;
pediatrics, obstetrics, and gynecology; dental; preventive medicine; internal
medicine and cardiology; maxillofacial surgery and neurosurgery; intensive
care beds and nursing; blood-banking service; pathology; infectious disease
services; medical nutrition therapy; behavioral health; occupational health;
medical logistics; and other medical specialties.

53
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Chapter 3
Tactical Combat Casualty Care
Medical Equipment
Tactical Combat Casualty Care-All Combatants (TCCC-AC) must be
familiar with the Improved First Aid Kit (IFAK)/Joint First Aid Kit (JFAK)
as well as other kits commonly seen in the force today. This chapter
discusses the equipment in Generation I and II IFAKs and other commonly
used rescue equipment: the Warrior Aid and Litter Kit (WALK), Skedco,
and for medics and Soldier familiarity, the M9 Medic Bag.
Improved First Aid Kit/Joint First Aid Kit
The IFAK Generation I is issued to every Service member at a Central Issue
Facility for administering immediate self-aid and buddy aid. Every Service
member must be trained in the use of all contents of the IFAK. The IFAK
does not contain a needle or angiocatheter for chest needle decompression.
All IFAK contents are described in the TCCC-AC training on the National
Association of Emergency Medical Technicians (NAEMT) website.
Figure 3-1. IFAK Generation I

54
CENTER FOR ARMY LESSONS LEARNED
Table 3-1. IFAK Generation I contents
National Stock No. Item No. Per Kit
8465-01-531-3647 100 Round Squad Automatic Weapon
(SAW)/Utility Pouch, MOLLE II
1
6515-01-521-7976 Combat Application Tourniquet 1
6510-01-460-0849 Bandage Kit, Elastic 1
6510-01-503-2117 Bandage Gauze, 4 1/2 inch, 100s 1
6510-00-926-8883 Surgical Adhesive Tape, 2 inch, 6s 1
6515-01-180-0467 Nasopharyngeal Airway 1
6515-01-519-9161 Patient Exam Gloves, 100s 4
6545-01-586-7691 Contents Kit, IFAK Resupply 1
6545-01-531-3147 Insert (Folding Panels With Cord) 1
6510-01-562-3325 Dressing, Combat Gauze 1
The Generation II IFAK is issued by the Rapid Fielding Initiative. This
IFAK includes two Combat Application Tourniquets, which are stored in
pouches that attach to the kit bag. The Generation II IFAK also contains a
vented chest seal and eye shield. The Generation II IFAK is similar to the
JFAK. Designers added Department of Defense (DD) Form 1380, Tactical
Combat Casualty Care (TCCC) Card, June 2014, a permanent marker,
and strap cutter. The kit weighs 1 pound and contains expendable medical
items. The Defense Medical Materiel Program Ofce is coordinating with
the Joint Services on the transition of the IFAK to the JFAK. The U.S. Navy
is currently the only Service utilizing needle chest decompression from the
JFAK.

55
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Figure 3-2. IFAK Generation II
Table 3-2. IFAK Generation II contents
National Stock No. Item No. Per Kit
6545-01-584-1582 U.S. Army IFAK 1
6515-01-521-7976 Combat Application Tourniquet 2
6510-01-492-2275 Bandage Kit, Elastic 1
6510-01-503-2117 Bandage, Gauze, 4 1/2 inch, 100s 1
6510-00-926-8883 Surgical Adhesive Tape, 2 inch, 6s 1
6515-01-180-0467 Nasopharyngeal Airway 1
6515-01-519-9161 Patient Exam Gloves, 100s 4
6510-01-562-3325 Dressing, Combat Gauze 1
4240-01-570-0319 Strap Cutter, Rescue 1
6510-01-549-0939 Bolin Chest Seal 1
6515-01-449-1016 Eye Shield, Fox 1
7520-00-312-6124 Marker, Tube Type 1

56
CENTER FOR ARMY LESSONS LEARNED
Warrior Aid and Litter Kit
The WALK (National Stock Number [NSN]: 6545-01-587-1199) offers an
option for a vehicle life-saving kit (see Figure 3-3).
The WALK allows rst-aid treatment and immediate evacuation of one
patient in a casualty evacuation (CASEVAC) vehicle and treatment of
multiple trauma patients at the point of injury (POI). The total weight of the
WALK is 29 pounds, 15 ounces.
The system holds the TALON II 90C quad-fold litter and a pocket-system
containing medical supplies (see Figure 3-4). The WALK contains a
Hypothermia Prevention and Management Kit (HPMK) to help stabilize
patients during transport. The WALK also includes the following:
• •
Five pairs Black Talon nitrile trauma gloves
• •
Two nasopharyngeal airways, size 28F with lubricant
• •
One casualty equipment bag
• •
Two HyFin chest seals
• •
Two ARS needle decompression kits, 14 gauge by 3.25 inch
• •
Two combat application tourniquets
• •
Six trauma dressings, 6 inch
• •
Four rolls of S-rolled gauze, 4.5 inch by 4.1 yards
• •
One abdominal emergency trauma dressing
• •
Two SAM Splint IIs
• •
One pair of trauma shears, 7.25 inch
• •
One roll surgical tape, 2 inch
• •
One role multipurpose tape
• •
Six polycarbonate eye shields
• •
One Combat Casualty Reference Card
• •
Two Combat Casualty Cards (Triage)
• •
One aviation panel (Recognition, Orange)
• •
Four tie-down straps (universal litter)

57
TACTICAL COMBAT CASUALTY CARE HANDBOOK
The WALK ts into any standard or nonstandard CASEVAC asset and
is useful as part of the prepositioning of medical supplies or cache on a
forward operating base, casualty collection point, or at a patrol base.
Figure 3-3. WALK

58
CENTER FOR ARMY LESSONS LEARNED
Figure 3-4. TALON II 90C quad-fold litter
Sked Basic Rescue System
The Sked (NSN: 6545-01-537-7904) is a semirigid litter that utilizes a sled
design to allow the evacuator to continue returning re as the casualty is
evacuated. It is used for conned space, high angle, or technical rescue and
provides patient protection while allowing the litter bearers to have their
hands free for weapons and security.
The Sked is equipped for horizontal hoisting by helicopter or vertical
hoisting in caves or industrial conned spaces. When the patient is
packaged, the litter becomes rigid. The Sked is rolled for storage in a
backpack, which is included with the system. The Sked litter system is 17
pounds.

59
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Figure 3-5. Sked
Figure 3-6. Casualty evacuation using the Sked

60
CENTER FOR ARMY LESSONS LEARNED
M9 Medical Aid Bag
The M9 Medical Aid Bag (NSN 6545-01-539-6448) is in the Department of
Defense inventory. It has been modied to decrease the silhouette of an aid
bag and the personnel carrying this product. Due to the variety of aid bags
available, the M9 is easily acquired and restocked by military logistics. This
bag can be utilized mounted or dismounted.
Figure 3-7. M9 Medical Aid Bag

61
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Figure 3-8. M9 Medical Aid Bag interior
Table 3-3. M9 Medical Aid Bag contents
National Stock No. Item No. Per
Kit
6545-01-572-9964 Medical Equipment Set (MES) Combat
Medic
1
4240-01-568-3219 Strap Cutter, Combat 1
6510-00-926-8884 Surgical Adhesive Tape 1
6510-00-935-5823 Elastic Bandage, 6 inch by 4.5 yards 4
6510-01-492-2275 Bandage Kit, Elastic 4
6510-01-503-2117 Bandage Gauze, 4.1 yards. 4
6510-01-519-8421 Occlusive Dressings, 5s 1
6510-01-519-9253 Surgical Sponges, 40s 1
6510-01-532-8930 Bandage, Elastic, 16 by 12 inches 1
6510-01-562-3325 Bandage Gauze, Impregnated 6
6510-01-571-9729 Compress and Bandage 2

62
CENTER FOR ARMY LESSONS LEARNED
Table 3-3. M9 Medical Aid Bag contents (continued)
National Stock No. Item No. Per
Kit
6510-01-573-0300 Chest Seal Dressing 4
6510-01-587-6579 Burn First Dressing 2
6515-00-9357138 Bandage Scissors 1
6515-01-314-6694 Stethoscope Comb, 28 inch 1
6515-01-449-1016 Rigid Eye Shield, Fox12 4
6515-01-494-1951 Universal Splint 2
6515-01-515-0151 Tool Kit Rescue Oropharyngeal Airway 1
6515-01-5162554 Easy Fit Suction Kit 1
6515-01-5163120 Easy Suction Catheter 1
6515-01-519-6764 Surgical Drainage Tubes, 6s 1
6515-01-521-3082 Pharyngeal Airway, 2s 2
6515-01-521-5730 Leg Splint 1
6515-01-5217976 Non-Pneumatic Tourniquet 6
6515-01-527-8068 Medical Head Lamp 1
6515-01-529-1187 Nasal Trumpet 3
6515-01-536-9363 Intraosseous Infusion 2
6515-01-540-7226 Trauma Leash Shears 2
6515-01-541-0635 Needle Decompression 2
6515-01-557-1136 Oximeter Pulse Port 1
6515-01-573-0692 Cricothyrotomy Set 2
6515-01-593-4841 Resuscitator, Hand Open 1
6532-01-524-6932 Survival Blanket 1
6532-01-525-4062 Heating Blankets, 8s 1
6545-01-539-6450 Medical Aid Bag 1
7520-00-312-6124 Marker, Tube Type 1
8345-01-573-3304 Panel Marker 1

63
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Chapter 4
MARCH/PAWS Treatment Algorithms
This chapter contains ow charts illustrating the proper use of Tactical
Combat Casualty Care (TCCC) principles of MARCH/PAWS and best
practices for conducting TCCC in a combat environment.
Figure 4-1

64
CENTER FOR ARMY LESSONS LEARNED
Figure 4-2

65
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Figure 4-3

66
CENTER FOR ARMY LESSONS LEARNED
Figure 4-4

67
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Figure 4-5

68
CENTER FOR ARMY LESSONS LEARNED
Figure 4-6

69
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Figure 4-7

71
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Chapter 5
Tactical Combat Casualty Care-All Combatants
Tactical Combat Casualty Care-All Combatants Training
The purpose of this chapter is to discuss training outcomes, provide
resources, and aid in the execution of Tactical Combat Casualty Care-All
Combatants (TCCC-AC). TCCC-AC is the TCCC course for non-medical
personnel. The National Association of Emergency Medical Technicians
(NAEMT) TCCC-AC training guidelines are standard for rst responder
training programs as stated by the Joint Trauma System and the Committee
on Tactical Combat Casualty Care (CoTCCC). Medical personnel are the
only authorized trainers for TCCC-AC courses. For guidelines, slides, and
additional TCCC information, visit NAEMT online at http://www.naemt.
org/education/TCCC/guidelines_curriculum or the Defense Health Agency
at http://www.health.mil/tccc.
TCCC-AC curriculum. The TCCC-AC slides have scenarios, practical
exercises, and videos. Instructor guides are available for each slide series.
• •
Conduct the TCCC-AC written pretest.
• •
View and review all slides with students.
• •
Conduct the TCCC-AC written posttest.
Skill station and practical exercises. The skills listed on the NAEMT
website are within the scope of practice for a non-medical Service member.
The NAEMT website provides documents for these skills, practical
exercises incorporating these skills, and an evaluation tool for these skills.
• •
Conduct TCCC-AC skill-set training.
• •
Conduct TCCC-AC skill-set validation testing.
• •
Conduct a practical exercise trauma lane (optional).
Instructors. TCCC-AC instructors are personnel who successfully
complete the Tactical Combat Casualty Care-Medical Provider (TCCC-MP)
course. The online NAEMT instructor course takes approximately 6 hours.
Upon completion, submit the NAEMT instructor application. An NAEMT
TCCC-afliate faculty member monitors the rst TCCC course taught.
TCCC-AC instruction is authorized in a 10:1 ratio according to CoTCCC
guidelines.

72
CENTER FOR ARMY LESSONS LEARNED
• •
The criterion for becoming a military TCCC instructor is being a
military medic, medical technician, corpsman, or other medical
personnel (ofcer or enlisted) trained to conduct medicine in the
Armed Services.
• •
Medical simulation and training centers are located at various
Army installations and may have NAEMT TCCC-afliate faculty
designation.
• •
The Defense Medical Readiness and Training Institute also has
NAEMT TCCC-afliate faculty staff and offer mobile training team
courses, which are listed on the Joint Knowledge Online website at
http://jko.jten.mil/.
Trauma lane. The CoTCCC allows additional lane training for TCCC. A
military operations on urbanized terrain (MOUT) or close-quarters combat
site can be utilized (for example, an ofce space, boat, ship, or fuselage)
that can offer realistic constraints (for example, difcult evacuation) to
render care to casualties.
Tactical Combat Casualty Care-All Combatants Skill Sets
As of 02 June 2014, the CoTCCC requires TCCC-AC rst responders to
have specic skill sets to perform the following:
• •
Massive hemorrhage:
Apply direct pressure to the hemorrhage.
Apply a bandage to the hemorrhage.
Apply a pressure dressing to the hemorrhage.
Apply a tourniquet to an extremity hemorrhage.
Apply combat gauze to the hemorrhage.
• •
Airway:
Demonstrate the chin lift/jaw thrust maneuver on a casualty.
Insert a nasopharyngeal airway (NPA) to a casualty.
Place a casualty in the recovery position.
Demonstrate the sit up/lean forward airway position on a casualty.
• •
Respirations: Treat a sucking chest wound with a vented chest seal.
• •
Circulation: Assess a casualty for shock.

73
TACTICAL COMBAT CASUALTY CARE HANDBOOK
• •
Head injury/hypothermia:
Package the casualty with a Hypothermia Prevention and
Management Kit (HPMK).
Treat penetrating eye injuries and demonstrate proper use of a
rigid eye shield.
Discuss the appropriate administration of oral moxioxacin.
• •
Casualty movement: Demonstrate effective casualty drags and manual
carries.
• •
TCCC medications:
Administer oral analgesics (Tylenol, meloxicam)
appropriately.
Administer oral antibiotics (moxioxacin) appropriately.
• •
Splinting:
Demonstrate effective application of a rigid eye shield.
Demonstrate effective limb splinting.
• •
Burns: Manage burns by stopping the burning process and covering
the casualty.
• •
Documentation: Correctly complete Department of Defense (DD)
Form 1380, Tactical Combat Casualty Care (TCCC) Card, June 2014,
for a casualty.
Tactical Combat Casualty Care-All Combatants Guidelines
Guidelines established by the CoTCCC are posted on the NAEMT website
at http://www.naemt.org/education/TCCC/tccc-ac. These recommendations
are intended to be guidelines only and are not a substitute for clinical
judgment.
Care Under Fire Basic Management Plan
• •
Return re and take cover.
• •
Direct or expect the casualty to remain engaged as a combatant, if
appropriate.
• •
Direct the casualty to move to cover and apply self-aid, if able.
• •
Try to keep the casualty from sustaining additional wounds.

74
CENTER FOR ARMY LESSONS LEARNED
• •
Massive hemorrhage: Stop any life-threatening external hemorrhage, if
tactically feasible:
Direct the casualty to control the hemorrhage by self-aid, if able.
Use a CoTCCC-recommended tourniquet for an extremity
hemorrhage.
Move the casualty to cover.
• •
Airway management is generally best deferred until the tactical eld
care (TFC) phase.
Tactical Field Care Basic Management Plan
NOTE: Casualties with an altered mental status should be disarmed
immediately.
• •
Massive hemorrhage:
Assess for an unrecognized hemorrhage and control all sources of
bleeding.
Use one or more CoTCCC-recommended limb tourniquets, if
necessary.
Use a CoTCCC-approved hemostatic dressing for compressible
hemorrhage not amenable to limb tourniquet use or as an adjunct
to tourniquet removal.
Immediately apply a CoTCCC-recommended junctional
tourniquet if the bleeding site is amenable to use of a junctional
tourniquet.
Reassess the prior tourniquet application:
•••*
Expose the wound and determine if a tourniquet is needed.
•••*
Replace any limb tourniquet placed over the uniform with
one applied directly to the skin, 2 to 3 inches above the
wound.
Expose and use an indelible marker to clearly mark all tourniquet
sites with the time of tourniquet application.
• •
Airway management:
Conduct the following for an unconscious casualty without an
airway obstruction:
•••*
Chin lift/jaw thrust maneuver.

75
TACTICAL COMBAT CASUALTY CARE HANDBOOK
•••*
NPA.
•••*
Place the casualty in the recovery position (see Figure 5-1).
Figure 5-1. Recovery position
Conduct the following for a casualty with an airway obstruction or
impending airway obstruction:
•••*
Chin lift/jaw thrust maneuver.
•••*
NPA.
•••*
Allow a conscious casualty to assume any position that best
protects the airway to include sitting up.
•••*
Place an unconscious casualty in the recovery position.
•••*
If these measures are unsuccessful, refer to a medic
immediately. Perform a surgical cricothyroidotomy using
one of the following:
•••••♦
CricKey technique.
•••••♦
Bougie-aided open surgical technique.
•••••♦
Standard open surgical technique.
•••••♦
Lidocaine, if the casualty is conscious.
• •
Respirations:
For a casualty with progressive respiratory distress and known or
suspected torso trauma, consider a tension pneumothorax.
All open and/or sucking chest wounds should be treated by:
•••*
Immediately applying a vented chest seal to cover the defect.

76
CENTER FOR ARMY LESSONS LEARNED
•••*
If a vented chest seal is not available, use a non-vented chest
seal.
•••*
Burping or temporarily removing the dressing. If this does
not relieve the respiratory distress, refer to a medic.
• •
Circulation:
Assess the casualty for hemorrhagic shock. If the casualty is not in
shock, oral uids are permissible if the casualty is conscious and
can swallow.
If the casualty is in shock, refer to a medic.
• •
Hypothermia prevention:
Minimize casualty environmental exposure and promote heat
retention.
Keep personal protective gear on, if feasible. Replace wet
clothing, if possible. Get the casualty onto an insulated surface as
soon as possible.
Use CoTCCC-approved hypothermia prevention kit, if available.
If a hypothermia prevention kit is not available, then use dry
blankets, poncho liners, sleeping bags, or anything that will retain
heat and keep the casualty warm and dry.
• •
Pain management: Analgesia on the battleeld should generally be
achieved by one of following options:
If there is mild to moderate pain and/or the casualty is able to
ght, give the casualty a TCCC combat wound pill pack (CWPP).
If there is moderate to severe pain and the casualty is not in shock,
refer to a medic.
• •
Antibiotics (recommended for all open combat wounds):
If the casualty can swallow, administer 400 milligrams (mg) of
moxioxacin from the CWPP.
If the casualty cannot swallow (shock or unconsciousness), refer
to a medic.
• •
Wounds:
Inspect and dress known wounds.
Check for additional wounds (for example, scalp lacerations).

77
TACTICAL COMBAT CASUALTY CARE HANDBOOK
• •
Splinting:
If a penetrating eye injury is noted or suspected, conduct the
following:
•••*
Cover the eye with a rigid eye shield and not a pressure
patch.
•••*
Administer 400 mg moxioxacin from the CWPP.
Splint fractures.
Tactical Evacuation Care Basic Management Plan
NOTE: In addition to reassessing the principles of tactical eld care (TFC),
perform manual carries as needed (Warrior Aid and Litter Kit [WALK] or
Sked).

79
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Chapter 6
Tactical Combat Casualty Care-Medical Provider
Tactical Combat Casualty Care-Medical Provider Training
The purpose of this chapter is to discuss training outcomes, provide
resources, and aid in the execution of Tactical Combat Casualty Care-
Medical Provider (TCCC-MP). The National Association of Emergency
Medical Technicians (NAEMT) TCCC-MP guidelines and training are
the standard for enlisted and ofcer TCCC medical personnel training as
stated by the Joint Trauma System and the Committee on Tactical Combat
Casualty Care (CoTCCC). Medical personnel are highly encouraged to
utilize the NAEMT TCCC-MP courses because they offer a credential
sponsored by the American College of Surgeons and 16 continuing
education hours. Visit the NAEMT website at http://www.naemt.org/
education/TCCC/guidelines_curriculum or the Defense Health Agency
website at http://www.health.mil/tccc for guidelines, slides, and additional
TCCC information.
TCCC-MP curriculum. The TCCC-MP slides have scenarios, practical
exercises, and videos. Instructor guides are available for each slide series.
• •
Conduct the TCCC-MP written pretest.
• •
View and review all slides with students.
• •
Conduct the TCCC-MP written posttest.
Skill station and practical exercises. The skills listed on the NAEMT
website are within the scope of practice for a medically trained Service
member. Located on the NAEMT site are documents for skills, practical
exercises incorporating these skills, and an evaluation tool for each skill.
• •
Conduct TCCC-MP skill-set training.
• •
Conduct TCCC-MP skill-set validation test.
• •
Conduct a practical exercise trauma lane (optional).
Instructors. TCCC-MP instructors are personnel who successfully
complete the TCCC-MP course, complete the 6-hour online NAEMT
instructor course, submit the NAEMT instructor application, and have an
NAEMT TCCC-afliate faculty member monitor during the rst TCCC
course taught. TCCC instruction must be given in a 4:1 ratio according to
NAEMT (Prehospital Trauma Life Support) guidelines.

80
CENTER FOR ARMY LESSONS LEARNED
• •
The criterion for becoming a military TCCC instructor is being any
military medic, medical technician, corpsman, or other medical
personnel (ofcer or enlisted) trained to conduct medicine in the
Armed Services.
• •
Medical Simulation and Training Centers are located at various
Army installations and may have NAEMT TCCC-afliate faculty
designation.
• •
The Defense Medical Readiness and Training Institute (DMRTI)
also has NAEMT TCCC-afliate faculty staff. DMRTI offers mobile
training team courses listed on Joint Knowledge Online website at
http://jko.jten.mil/.
Trauma lane. CoTCCC allows additional lane training for TCCC. A
conned space can be utilized (for example, an ofce space, boat, ship,
or fuselage) that can offer realistic constraints (for example, difcult
evacuation) to render care to casualties.
Tactical Combat Casualty Care-Medical Provider Skill Set
As of 02 June 2014, the CoTCCC requires TCCC-MP medical enlisted
personnel (medics, medical technicians, corpsmen, medical ofcers, or
operating room special operations medics) to have specic skill sets to
perform the following (unless otherwise noted):
• •
Massive hemorrhage:
Apply direct pressure to the hemorrhage.
Apply a bandage to the hemorrhage.
Apply a pressure dressing to the hemorrhage.
Apply a tourniquet to an extremity hemorrhage.
Apply Combat Gauze to the hemorrhage.
Apply a pelvic splint.
• •
Airway:
Demonstrate the chin lift/jaw thrust maneuver on a casualty.
Insert a nasopharyngeal airway (NPA) to a casualty.
Place a casualty in the recovery position.
Demonstrate the sit up/lean forward airway position on a casualty.

81
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Demonstrate the insertion of a supraglottic airway.
Demonstrate a surgical airway (cricothyroidotomy).
Demonstrate endotracheal intubation (medical ofcers and
operating room special operations medics).
• •
Respirations:
Treat a sucking chest wound with a chest seal.
Demonstrate a needle chest decompression (NCD).
Demonstrate insertion of a chest tube (medical ofcers and
operating room special operations medics).
Demonstrate oxygen administration.
• •
Circulation:
Assess for shock.
Initiate an intravenous (IV) access/saline lock.
Initiate an intraosseous (IO) access.
Demonstrate IV/IO uid resuscitation.
Demonstrate the use of IV/IO analgesics.
Demonstrate the use of IV/IO tranexamic acid (TXA).
Demonstrate the use of IV/IO antibiotics.
Demonstrate the use of IV/IO blood product administration
(medical ofcers and operating room special operations medics).
• •
Head injury/hypothermia:
Demonstrate the Hypothermia Prevention and Management Kit
(HPMK).
Treat penetrating eye injuries:
•••*
Demonstrate the proper use of a rigid eye shield.
•••*
Discuss appropriate administration of oral moxioxacin.
• •
Casualty movement: Demonstrate effective casualty drags, manual
carries, use of a Talon litter (in the Warrior Aid and Litter Kit
[WALK]) and Sked stretcher.

82
CENTER FOR ARMY LESSONS LEARNED
• •
TCCC medications:
Administer oral analgesics (Tylenol, moxioxacin) appropriately.
Administer oral antibiotics appropriately.
Administer oral transmucosal fentanyl citrate (OTFC)
appropriately.
Administer intramuscular (IM) antibiotics appropriately.
Administer intranasal (IN), IM, IV, or IO ketamine appropriately.
Administer IV or IO morphine appropriately.
• •
Fractures:
Demonstrate effective splinting with a rigid eye shield.
Demonstrate effective splinting with a pelvic splint.
Demonstrate effective limb splinting.
• •
Burns:
Manage burns by stopping the burning process and covering the
casualty.
Cover the burn injuries.
Initiate the burn-uid resuscitation procedures.
• •
Documentation: Correctly complete Department of Defense (DD)
Form 1380, Tactical Combat Casualty Care (TCCC) Card, June 2014.
• •
Monitoring: Demonstrate the use of mission-appropriate electronic
monitoring devices (pulse oximeter, Zoll monitor/debrillator,
Propaqmonitor, etc.).

83
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Tactical Combat Casualty Care-Medical Provider Guidelines
As of 11 November 2015, the guidelines established by the CoTCCC are
posted on the NAEMT website at http://www.naemt.org/education/TCCC/
tccc-ac. These recommendations are intended to be guidelines only and are
not a substitute for clinical judgment.
Care Under Fire Basic Management Plan
• •
Return re and take cover.
• •
Direct or expect the casualty to remain engaged as a combatant, if
appropriate.
• •
Direct the casualty to move to cover and apply self-aid, if able.
• •
Keep the casualty from sustaining additional wounds.
• •
Massive hemorrhage:
Stop a life-threatening external hemorrhage, if tactically feasible.
Direct the casualty to control the hemorrhage by self-aid, if
possible.
Use a CoTCCC-recommended tourniquet for an extremity
hemorrhage.
Move the casualty to cover.
• •
Airway management is generally best deferred until the tactical eld
care (TFC) phase.
Tactical Field Care Basic Management Plan
NOTE: Casualties with an altered mental status should be disarmed
immediately.
• •
Massive hemorrhage:
Assess the casualty for an unrecognized hemorrhage and control
all sources of the bleeding.
Use one or more CoTCCC-recommended limb tourniquets, if
necessary.

84
CENTER FOR ARMY LESSONS LEARNED
Use a CoTCCC-approved hemostatic dressing for a compressible
hemorrhage not amenable to a limb tourniquet use or as an
adjunct to tourniquet removal:
•••*
Combat Gauze, Celox Gauze, or ChitoGauze (abdomen or
pelvis).
•••*
Special Operations Forces only: XStat sponges (deep,
narrow-tract, junctional wounds).
Immediately apply a CoTCCC-recommended junctional
tourniquet if the bleeding site is amenable to use of a junctional
tourniquet.
Reassess the prior tourniquet application by doing the following:
•••*
Expose the wound and determine if a tourniquet is needed.
•••*
Replace any limb tourniquet placed over the uniform with
one applied directly to the skin, 2 to 3 inches above the
wound.
• •
Airway management:
For an unconscious casualty without airway obstruction, perform
the following:
•••*
Chin lift/jaw thrust maneuver.
•••*
NPA.
•••*
Place the casualty in the recovery position (see Figure 6-1).
Figure 6-1. Recovery position
For a casualty with an airway obstruction or impending airway
obstruction, perform the following:
•••*
Chin lift/jaw thrust maneuver.
•••*
NPA.

85
TACTICAL COMBAT CASUALTY CARE HANDBOOK
•••*
Allow a conscious casualty to assume any position that best
protects the airway to include sitting up.
•••*
Place an unconscious casualty in the recovery position.
• •
Respiration:
For a casualty with progressive respiratory distress and known
or suspected torso trauma, consider a tension pneumothorax and
NCD on the side of the injury:
•••*
Remove the plastic cap from the 3.25 inch, 14-gauge needle.
•••*
Insert the needle into the skin over the superior border of the
third rib, mid-clavicular line, and direct the needle into the
second intercostal space at a 90 degree angle.
•••*
As the needle enters the pleural space, a “pop” will be felt. If
a “hiss” of air is heard, ensure that the needle is advanced all
the way to the hub.
•••*
Remove the needle, leaving the catheter in place.
•••*
Stabilize the catheter hub to the chest wall with 1/2 inch
gauze tape.
Each open and/or sucking chest wound is treated by:
•••*
Immediately applying a vented chest seal to cover the defect.
•••*
If a vented chest seal is not available, use a non-vented chest
seal.
•••*
If respiratory distress ensues, burp or temporarily remove the
dressing. If there is no improvement, consider an NCD.
• •
Circulation:
Control of bleeding takes precedence over infusing uids. Start an
18-gauge IV or saline lock, if indicated.
An IO device is an alternative route for administering uids when
uid resuscitation is required and IV access cannot be obtained.
Give 1 gm of TXA as soon as feasible to casualties in or at risk of
hemorrhagic shock.

86
CENTER FOR ARMY LESSONS LEARNED
Clinical signs of shock on the battleeld are (1) unconsciousness
or altered mental status not due to coexisting traumatic brain
injury (TBI) or drug therapy, and/or (2) abnormal radial pulse.
If the casualty is not in shock, oral uids are permissible if
the casualty is conscious and can swallow. If the casualty is
in shock, resuscitate with whole blood, freeze-dried plasma,
or 500 milliliter (ml) bolus of Hextend. The casualty should
then be observed for 30 minutes. If there is insufcient clinical
improvement, a second 500 mL bolus of Hextend should then be
administered in a similar manner. Do not administer more than
1,000 ml of Hextend.
Convert limb tourniquets and junctional tourniquets if the
following three criteria are met:
•••*
The casualty is not in shock.
•••*
It is possible to monitor the wound closely for bleeding.
•••*
The tourniquet is not being used to control bleeding from an
amputation.
Do not attempt to remove a tourniquet if the anticipated
evacuation time is less than 2 hours or the casualty is in shock.
Resuscitate the casualty frequently until there is a palpable radial
pulse, improved mental status, or a systolic blood pressure (SBP)
of 90 millimeter of mercury (mmHG) is present. Discontinue
uids when one or more points are achieved.
Reassess the casualty every 15 minutes for recurrence of shock. If
shock recurs, verify all hemorrhages are under control and repeat
uid resuscitation as above.
• •
Hypothermia prevention:
Minimize casualty environmental exposure and promote heat
retention.
Keep personal protective gear on, if feasible. Replace wet
clothing, if possible. Get the casualty onto an insulated surface as
soon as possible. Use CoTCCC-approved hypothermia prevention
kit, if available. If not available, use dry blankets, poncho liners,
sleeping bags, or any heat-retaining item and keep the casualty
warm and dry.
Warm IV uids, if possible.

87
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Casualties with both shock and TBI should receive IV or IO uids
until the radial pulse is restored, which corresponds to an SBP of
approximately 70 mmHg.
• •
Pain management:
Analgesia on the battleeld should generally be achieved by one
of the three following options:
•••*
If there is mild to moderate pain and/or the casualty is able
to ght, give the casualty the TCCC combat wound pill pack
(CWPP).
•••*
If there is moderate to severe pain and the casualty is not in
shock, administer 800 micrograms (mcg) of OTFC.
•••*
If there is moderate to severe pain and the casualty is in
shock, administer 50 milligrams (mg) of ketamine IM
or IN every 30 minutes, as needed, or administer 20 mg
of ketamine by slow IV or IO push every 20 minutes, as
needed.
NOTE: The endpoint control of pain for ketamine is an eye
nystagmus. Consider 4 mg of ondansetron (Zofran) by IV, IO, or
IM every 8 hours for nausea and vomiting.
• •
Antibiotics: Antibiotics are recommended for all open combat wounds.
If the casualty can swallow, administer 400 mg of moxioxacin,
from the combat wound pill pack (CWPP).
If the casualty cannot swallow (because of shock or if
unconsciousness), administer 1 gram (gm) ertapenem (Invanz) by
IV or IM.
• •
Wounds:
Inspect and dress known wounds.
Check for additional wounds (for example, scalp lacerations).
• •
Splinting:
Conduct the following for splinting a penetrating eye trauma:
•••*
Perform a rapid eld test of the casualty’s visual acuity.
•••*
Cover the eye with a rigid eye shield and not a pressure
patch.

88
CENTER FOR ARMY LESSONS LEARNED
•••*
Administer 400 mg moxioxacin from the CWPP if the
casualty can swallow. If the casualty cannot swallow,
administer IV or IM antibiotics.
For fractures, apply a pelvic splint for lower extremity traumatic
amputation, vehicle rollover, or building collapse.
• •
Monitoring: Utilize pulse oximetry as an adjunct to clinical
monitoring.
• •
Communication and documentation: Communicate with the casualty
and the next higher Role of care. Use the TCCC Casualty Card to
record care. The TCCC Card is formatted in the MIST (mechanism
of injury, injuries, signs/symptoms, and treatment) Report. The MIST
Report is a standardized patient hand-over.
• •
Cardiopulmonary resuscitation (CPR):
Battleeld blast or penetrating trauma casualties with no pulse, no
respirations, and no other signs of life should not be resuscitated.
Casualties with torso trauma or polytrauma and no pulse or
respirations should have bilateral NCD performed to conrm or
deny pneumothorax prior to discontinuing resuscitation.
• •
Burns:
Facial burns should be aggressively monitored for airway status
and potential inhalation injury.
Estimate total body surface area (TBSA) burned to the nearest 10
percent, utilizing the Rule of Nines. (See Figure 6-2.)

89
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Rule of Nines
Estimate the TBSA that has been burned on an adult by using multiples
of 9. The percentage of the body involved can be calculated as follows:
Head = 9%
Chest (front) = 9%
Abdomen (front) = 9%
Upper/mid/low back and buttocks = 18%
Each arm = 9% (front = 4.5%, back = 4.5%)
Groin = 1%
Each leg = 18% total (front = 9%, back = 9%)
Figure 6-2. Rule of Nines
Cover burned areas with dry, sterile dressings. For burns over 20
percent TBSA, consider placing the casualty into an HPMK, body
bag, or alternative.
United States Army Institute of Surgical Research Rule of Ten
uid resuscitation (calculate the TBSA of the burns to the nearest
10 percent):
•••*
For burns over 20 percent of TBSA, initiate IV or IO uids
as soon as possible with lactated Ringers (LR), normal saline
(NS), or Hextend solution.
•••*
If Hextend solution is used, use no more than 1,000 ml
followed by LR or NS, as needed.
Tactical Evacuation Care Basic Management Plan
NOTE: In addition to the principles of tactical eld care (TFC), consider
the following for tactical evacuation care:
• •
Massive hemorrhage: Continually reassess all tourniquets and
bandages for bleeding from vehicular vibrations.

90
CENTER FOR ARMY LESSONS LEARNED
• •
Airway management: Consider the following for a casualty with a
current or impending airway obstruction:
Supraglottic airway (King LT, iGel, etc.).
Endotracheal intubation (suction, Tube Tamer, bag-valve mask,
bougie, GlideScope).
• •
Respirations:
Consider a chest tube insertion if the casualty has no improvement
and/or if a long transport is anticipated.
Administer oxygen when possible for the following types of
casualties:
•••*
Low oxygen saturation by pulse oximetry (shock, chest
wound, etc.).
•••*
Injuries associated with impaired oxygenation.
•••*
An unconscious casualty.
•••*
A casualty with TBI (maintain oxygen saturation over 90
percent).
•••*
Casualty at altitude (over 5,000 feet above sea level).
• •
Circulation: Continuously reassess IV or IO access for patency and
security.
• •
Head injury/hypothermia:
Casualties with moderate to severe (penetrating) TBI should be
monitored for:
•••*
Decreases in level of consciousness.
•••*
Pupillary dilation.
•••*
SBP over 90 mmHg or mean arterial pressure over 60.
•••*
Oxygen saturation (pulse oximetry) over 90 percent.
•••*
Hypothermia (core temperature under 96 F [35.5 C]).
•••*
Partial pressure of carbon dioxide (if capnography is
available, maintained between 35 to 40 mmHg).

91
TACTICAL COMBAT CASUALTY CARE HANDBOOK
•••*
For a penetrating head trauma, administer antibiotics
(ertapenam, 1 gm).
•••*
Assume a C-spine injury until cleared.
If impending herniation is suspected, take the following actions:
•••*
Administer 250 ml of 3 percent or 5 percent hypertonic
saline bolus by IV or IO.
•••*
Elevate the casualty’s head 30 degrees.
•••*
Control pain even in an unconscious patient (no morphine).
•••*
Hyperventilate the casualty (bag-valve mask ventilation rate
of 14 to 20).
Package the casualty in an HPMK or equivalent Blizzard Survival
Blanket, poncho, sleeping bag, etc.

93
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Appendix A
Tactical Combat Casualty Care Card
Figure A-1. TCCC Card (front)

94
CENTER FOR ARMY LESSONS LEARNED
Figure A-2. TCCC Card (back)

95
TACTICAL COMBAT CASUALTY CARE HANDBOOK
NOTE: Department of Defense (DD) Form 1380, Tactical Combat Casualty
Care (TCCC) Card, June 2014, is displayed in the MIST (mechanism of
injury, injuries, signs/symptoms, and treatment) Report format. The MIST
Report is the “debrief” or patient handover report for the next Role of care
or evacuation platform attendant (ight medic, ground ambulance medic, en
route critical care nurse).
NOTE: Change occurs with metrics. Metrics are created from data. Data
must be documented.

97
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Appendix B
Tactical Combat Casualty Care
After Action Report
The Tactical Combat Casualty Care (TCCC) After Action Report (AAR)
is to be completed within 72 hours of the injury occurring by the point of
injury (POI) medical team or Role I care and sent to the Department of
Defense Trauma Registry (DODTR).
The DODTR is the data repository for Department of Defense (DOD)
trauma-related injuries. The goal of this registry is to document, in
electronic format, information about the demographics, injury-producing
incident, diagnosis and treatment, and outcome of injuries sustained by
U.S./non-U.S. military and U.S./non-U.S. civilian personnel in wartime
and peacetime from the point of wounding to nal disposition. The Joint
Trauma System (JTS) collects data from Department of Defense (DD) Form
1380, Tactical Combat Casualty Care (TCCC) Card, June 2014; TCCC
AARs; and from the Armed Forces Medical Examiner Services (AFMES).
Documentation is vital to accumulate data in the DODTR, formerly the
Joint Theater Trauma Registry. JTS functions include the following:
• •
JTS Operations: The Data Acquisition division mines medical records
to abstract, code, and enter critical trauma data into the DODTR
database. The Data Analysis division develops, queries, and provides
data from the DODTR in response to requests for information
and conducts classied and nonclassied data analysis. The Data
Automation division supports information technology for the DODTR
and data-related special projects.
• •
Trauma Care Delivery maintains a database of operational and
physiologic parameters related to delivery of en route care and has
evaluated the validity of the “golden-hour” standard for movement
of casualties from POI to the rst surgical capability. The addition of
a military en route care registry (MERCuRY database) captures all
ground, air, and ship transport care.
• •
Performance Improvement coordinates improvement activities across
the spectrum of trauma care developing Performance Improvement
course content and training for combatant command trauma system
development.

98
CENTER FOR ARMY LESSONS LEARNED
Figure B-1. TCCC AAR (front)

99
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Figure B-2. TCCC AAR (back)

101
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Appendix C
Medical Triage Categories
Triage
Triage will be performed at all levels. Traditional categories of triage are
immediate, delayed, minimal, and expectant. To easily remember the order
of the categories, use the acronym IDME. No signicant treatment should
occur in the triage area. Casualties should be rapidly sent to the appropriate
treatment area for care.
Immediate. This group requires attention within minutes to 2 hours upon
arrival to avoid death or major disability. Injuries include airway obstruction
or potential compromise, tension pneumothorax, uncontrolled hemorrhage,
threatened loss of limb, or multiple extremity amputations.
Delayed. This group includes those wounded who are in need of surgery,
but whose general condition permits delay in treatment without unduly
endangering life, limb, or eyesight. Injuries include blunt or penetrating
torso injuries, fractures, soft-tissue injuries, facial fractures without airway
compromise, globe injuries, or survivable burns.
Minimal. This group has relatively minor injuries (e.g., minor lacerations,
abrasions, fractures of small bones, and minor burns) and can effectively
care for themselves with minimal medical care. These casualties may also
provide manpower to assist with movement or care of the injured. Such
casualties may inundate the facility, leading to early commitment and
ineffective utilization of resources. It is imperative to secure and strictly
control access to the military treatment facility (MTF) immediately upon
notication of a mass casualty event.
Expectant. This group has injuries that overwhelm current medical
resources at the expense of treating salvageable patients. The expectant
casualty should not be abandoned, but should be separated from the view
of other casualties and intermittently reassessed. These casualties require
a staff capable of monitoring and providing comfort measures. Injuries
include absent vital signs or signs of life, transcranial gunshot wound,
open pelvic injuries with uncontrolled bleeding and Class IV shock, burns
without reasonable chance for survival or recovery, or high spinal cord
injuries.

102
CENTER FOR ARMY LESSONS LEARNED
Mass Casualty
A mass casualty (MASCAL) event overwhelms any immediately available
medical capabilities to include personnel, supplies, and/or equipment.
Effective MASCAL response is founded on the principle of triage, the
system of sorting and prioritizing casualties based on the tactical situation,
mission, and available resources.
Mass Casualty Planning
Supplies. Class VIII medical supplies include equipment, drugs, oxygen,
dressings, sutures, sterilization capability, blood, etc. Immediate liaison with
the logistics system in the MTF and the theater of operation is essential to
ensure available and timely resupply. Class VIII boxes should be placed
near planned casualty collection points.
Personnel. Know the professional capability of personnel. Be prepared
to divert casualties to another facility. A response plan should include
personnel recall.
Capability. Know the number of operating room and intensive care unit
beds, holding capacity, and available diagnostic equipment (ultrasound,
X-ray, computed tomography [CT] scan, and laboratory tests).
Communication is essential among the MASCAL team, litter bearers,
higher command, and neighboring facilities.
Walking Blood Bank
Massively transfused casualties (over 10 units of red blood cell count [RBC]
in 24 hours) have a high mortality rate (33 percent) and have the greatest
potential to benet from appropriate transfusion strategies. Retrospective
cohort studies of casualties requiring massive transfusions during Operation
Enduring Freedom (OEF) and Operation Iraqi Freedom (OIF) demonstrate
a signicant survival benet for the massively transfused casualty when
RBC, fresh frozen plasma, and platelets are transfused at a 1:1:1 ratio. Fresh
whole blood (FWB) is available in austere conditions as a walking blood
bank (WBB) program that can be established based on a risk assessment
and the potential for casualties. FWB has no loss of clotting factors or
platelet activity.
FWB risks. There are risks associated with the use of FWB, including
increased risk of transfusion-transmitted infections (e.g., human
immunodeciency virus [HIV], hepatitis B and C, syphilis), a period of
decreased exercise tolerance in donors (mission effect on casualty’s unit),
and an increased risk of clerical errors (ABO typing) due to the potentially
chaotic activity during which FWB is requested. Additionally, eld
conditions are inherently unsanitary and are presumed to increase the risk of
bacterial contamination of the blood.

103
TACTICAL COMBAT CASUALTY CARE HANDBOOK
WBB planning. Coordination with the area joint blood program ofcer is
required to establish a WBB program. Prescreened donors registered into
the WBB program are preferably composed of active duty, active Reserve,
active National Guard, and other Department of Defense beneciaries.
Coalition forces will not be utilized routinely because donors and foreign
nationals are used as a last resort.
Donor FWB must be an ABO type-specic match to the casualty. If not
matched, a fatal hemolytic reaction may occur. Type O whole blood is
not universal. For more information see the Joint Theater Trauma System
clinical practice guideline found online at http://www.usaisr.amedd.army.
mil/cpgs/Fresh_Whole_Blood_Transfusion_24_Oct_12.pdf.

105
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Appendix D
Medical Evacuation Precedence Categories
Evacuation Categories
The more severe casualties (urgent and urgent-surgery precedence
casualties) should be evacuated before priority or routine precedence
casualties. Every effort should be made to staff and equip non-medical
vehicles used for casualty evacuation (CASEVAC) with medical personnel,
even if only to move the routine patient precedence category. NOTE:
Priority I through IV are NATO terms. NATO Standard Agreement 3204,
Aeromedical Evacuation, has deleted the Priority IV category.
Evacuation Priority
Priority is established by the treatment element or the senior military
medical person. Soldiers are evacuated based on their medical condition,
assigned evacuation precedence, and availability of medical evacuation
platforms.
Priority I Urgent is assigned to emergency cases that should be evacuated
as soon as possible and within a maximum of 1 hour in order to save life,
limb, or eyesight to prevent complications of serious illness or to avoid
permanent disability.
Priority IA Urgent Surgical is assigned to patients who must receive far
forward surgical intervention to save life and to stabilize them for further
evacuation.
Priority II Priority is assigned to sick and wounded personnel requiring
prompt medical care. This precedence is used when the individual should
be evacuated within four hours or his medical condition could deteriorate
to such a degree that he will become an urgent precedence, or whose
requirements for special treatment are not available locally, or will suffer
unnecessary pain or disability.
Priority III Routine is assigned to sick and wounded personnel requiring
evacuation but whose condition is not expected to deteriorate signicantly.
The sick and wounded in this category should be evacuated within 24 hours.
Priority IV Convenience is assigned to patients for whom evacuation by
medical platform is a matter of medical convenience rather than necessity.

106
CENTER FOR ARMY LESSONS LEARNED
Helicopter Landing Zone
Aircraft normally approach a tactical landing site without the aid of the
search landing light. The inverted “Y” system is used as the primary
marking for U.S. Forces. There is no landing zone (LZ) marking for
day operations, except smoke. Tactical lighting of the LZ can consist of
Chemlights, “beanbag” lights on the ground, or a Chemlight attached to a
550 cord, swung in a circular motion. A lighted inverted “Y” indicates the
landing point of the lead helicopter.
Figure D-1. Inverted “Y” system

107
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Appendix E
9-Line Request With MIST Report
Figure E-1. 9-Line Request with MIST Report

108
CENTER FOR ARMY LESSONS LEARNED
NOTE: The 9-Line Request includes a MIST (mechanism of injury,
injuries, signs/symptoms, and treatment) Report. Multiple casualties can be
used on a single 9-Line Report, and one casualty is used per MIST Report.

109
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Appendix F
Prolonged Field Care
The NATO denition of prolonged eld care (PFC) is eld medical care
applied beyond “doctrinal planning time lines” in order to decrease patient
mortality and morbidity. PFC utilizes limited resources and is sustained
until the patient arrives at the next appropriate level of care. For more
information see the Special Operations Medical Association website at
http://www.specialoperationsMedicine.org/Pages/pfcresources.aspx.
Special Operations Command
The Special Operations Command (SOCOM) Prolonged Field Care
Working Group (PFCWG) emphasizes basic medical skills that, when put
together, allow for a more comprehensive approach to critical patient care in
an austere setting.
Prolonged Field Care Capabilities
There are 10 PFC capabilities:
• •
Monitor the patient to create a useful vital-signs trend.
• •
Resuscitate the patient beyond crystalloid or colloid infusion (blood
products).
• •
Ventilate or oxygenate the patient (positive end-expiratory pressure
[PEEP], ventilator, supplemental oxygen).
• •
Gain denitive control of the patient’s airway (cricothyrotomy, rapid
sequence intubation, and endotracheal tube).
• •
Use sedation or pain control (intravenous [IV] sedation, ketamine,
Versed, fentanyl, etc.).
• •
Use physical examination or diagnostic measures (ultrasound,
diagnostic peritoneal lavage, laboratory testing).
• •
Provide nursing, hygiene, or comfort measures (wound care and
catheterizations).
• •
Perform advanced surgical interventions (chest tube, cricothyrotomy,
fasciotomy, amputation).
• •
Perform a telemedicine consult (media to transfer trends, images, lab
results).

110
CENTER FOR ARMY LESSONS LEARNED
• •
Prepare the patient for ight (basic ight physiology, Joint Enabling
Capabilities Command [JECC], Critical Care Air Transport Team
[CCATT], ight surgeon).
Tourniquet Conversion
The emphasis on hemorrhage control has and will continue to result in the
application of tourniquets. As soon as tactically allowable, all tourniquets
must be reassessed for conversion. Consider the following guidelines when
addressing tourniquet conversion:
• •
Less than two hours after the application is considered safe (attempt
conversion).
• •
Two to six hours is likely safe, but the upper safe limit has not been
scientically determined (attempt conversion).
• •
More than six hours requires caution (eld conversion not advised).

111
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Appendix G
Drug Reference Guide
Tactical Combat Casualty Care-Medical Provider (TCCC-MP) medications
are referenced throughout the TCCC-MP guidelines, skill sets, and
algorithms. These medications are described below:
• •
Acetaminophen (Tylenol), 625 milligram (mg) bilayer caplet.
Indications are mild to moderate pain in a conscious casualty able to
swallow. A typical dose is two tablets every 8 hours. (Available in the
Tactical Combat Medical Care Medical Equipment Set [MES].)
• •
Cefotetan, 2 grams (gm), intravenous (IV) antibiotic. Indication is
traumatic injury.
• •
Diazepam (Valium), 5 mg/2 milliliter (ml) injection. Indications are
rapid sequence induction, current or anticipated seizure activity, or
sedative for combative casualty. (Available in both the Combat Medic
and Tactical Combat Medical Care MES.)
• •
Ertapenam (Invanz), 1 gm IV antibiotic. Indication is traumatic injury.
• •
Fentanyl citrate, transmucosal lozenge (oral transmucosal fentanyl
citrate [OTFC]), 800 micrograms (mcg). Indications are moderate
to severe pain in a conscious casualty able place the lozenge in the
mouth. Tape the lozenge to the casualty’s index nger and direct it
into the mouth. Advise casualty not bite and/or swallow the lozenge.
(Available in the Combat Medic MES.)
• •
Flumazenil (Romazicon), 0.4 mg injection every 15 minutes.
Indications are as reversal agent for benzodiazepines (Diazepam
[Valium]). (Available in the Tactical Combat Medical Care MES.)
• •
Hetastarch, 500 ml IV bag. Indications are hemorrhage or burns.
(Available in both the Combat Medic and Tactical Combat Medical
Care MES.)
• •
Ketamine injection, 10 ml vial. Indications are moderate to severe
pain in a conscious or unconscious casualty. Deliver intranasal, 50
mg; or IV; intramuscular (IM); or intraosseous infusion (IO), 20 mg.
(Available in both the Combat Medic and Tactical Combat Medical
Care MES.)
• •
Meloxicam, oral tablets, 15 mg. Indications are mild to moderate pain
in a conscious casualty able to swallow. (Available in both the Combat
Medic and Tactical Combat Medical Care MES.)

112
CENTER FOR ARMY LESSONS LEARNED
• •
Moxioxicin, 400 mg oral tablet antibiotic. Indications are eye injury
or other traumatic injury. Casualty must be conscious and able to
swallow. (Available in both the Combat Medic and Tactical Combat
Medical Care MES.)
• •
Naloxone hydrochloride (Narcan), 1 mg/2 ml. Indication is as reversal
agent for opioids (OTFC, morphine, heroin, and limited reversal of
ketamine). (Available in both the Combat Medic and Tactical Combat
Medical Care MES.)
• •
Ondansetron (Zofran), oral disintegrating tablets, 4 mg rapid release.
Indication is anti-emetic (nausea and vomiting prevention) from opioid
administration. (Available in the Combat Medic MES.)
• •
Sodium chloride, 10 ml injection. Indications are IV or IO ush
(500 ml or 1,000 ml normal saline is an alternative IV uid). Three
percent sodium chloride is a hypertonic solution for the treatment of
increased intracranial pressures. (Available in both the Combat Medic
and Tactical Combat Medical Care MES.)
• •
Tranexamic acid (TXA), 1 gm IV piggyback with 100 ml normal
saline, lactated Ringers or Hextend solution. Indications are
excessive hemorrhage, given within three hours of injury. TXA is
an antibrinolytic agent. (Available in both the Combat Medic and
Tactical Combat Medical Care MES.)

113
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Appendix H
Medical Transition Guidelines in a
Tactical Environment
The predeployment site survey is the initial contact on the ground made
between an element of the incoming and the current unit in theater. The
relief in place (RIP) and a transfer of authority (TOA), from the outgoing
medical teams to the incoming medical teams, occurs when the entirety of
units transition. Done correctly, the RIP and TOA allow the departing team
to conduct a handover to the incoming team with minimal interruption. The
following are key areas that should be addressed during the RIP and TOA.
They may apply to the incoming team, outgoing team, or both.
• •
Transport and evacuation vehicle and equipment training, to include
routes, forward operating base regulations, and security coordination.
• •
Medical property accountability and property book transfer.
• •
Theater-unique medical briengs and policies. This may include
medical concept of operations, medical rules of engagement, and
current trends or projects completed and pending.
• •
Key leader engagements:
Medical. Subordinate and higher medical teams, contractor
medical teams, forward surgical teams, Special Operations
Forces medical teams, partner-nation medical teams, and medical
logistics personnel.
Operations. Aviation units, personal security detachment medics,
contract medical advisors, personnel recovery teams, national
security force development teams, nongovernmental agencies, or
governmental agencies.
• •
Orientation of forward operating base facilities.
• •
Emergency response plan process and mass casualty plan with review
and rehearsal of casualty collection points.
• •
Communications support (Transportation Command Regulating and
Command and Control Evaluation System [TRAC2ES], Medical
Protection System [MEDPROS], Armed Forces Health Longitudinal
Technology Application [AHLTA] Warrior, AHLTA Theater, etc.) and
equipment orientation for both unclassied and classied computer
networks.

114
CENTER FOR ARMY LESSONS LEARNED
• •
Battle rhythm (section, Role I, patient evacuation coordination cell
meetings, force protection meeting, medical development, Chief of
Staff meeting, Purple Heart committee, etc.).
• •
Orders and reporting processes and requirements (mild traumatic brain
injury, epidemiology, death, serious incident report, wake criteria,
battle injury tracker, casualty evacuation trends, Tactical Combat
Casualty Care after action report, operation orders, fragmentary orders,
etc.).
• •
Awards, badges, policy letters, and appointment orders orientation
(Purple Hearts, Combat Medic Badge).

115
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Appendix I
Medical planning and relief in place (RIP)/transfer of authority (TOA)
coordination focuses around the following U.S. Army Medical Department
(AMEDD) functions:
• •
Medical evacuation (MEDEVAC) and medical regulating entails
collecting, sorting, transporting, and providing en-route medical care.
Patients are evacuated from the lower level by the higher level of care.
The use of dedicated MEDEVAC assets may not be possible. The
medical planner must integrate the use of non-medical, nonstandard
evacuation assets (casualty evacuation [CASEVAC]) into the
MEDEVAC plan. To accomplish the MEDEVAC mission in hostile or
denied areas, operational security dictates that the mission airframes
used for the extraction of the force are used to transport patients.
• •
Medical regulating is the coordination and control of moving patients
to military treatment facilities (MTFs) best able to provide the required
specialty care. This system is designed to ensure the efcient and safe
movement of patients, identifying those patients awaiting evacuation,
locating available beds, and coordinating transportation means for
movement. Control of patient evacuation to appropriate hospitals
ensures adequate beds are available for current and anticipated needs
and moving patients requiring specialized treatment to the appropriate
MTF.
• •
Medical treatment consists of those measures necessary to recover,
resuscitate, stabilize, and prepare the casualty for evacuation. It also
includes routine sick call and care of minor illness or injury. For those
units that do not have organic Level I and Level II care capabilities,
medical treatment is provided on an area support basis. Entry into
immature and austere theaters causes unique challenges for medical
coverage.
Sick call provides the daily care for routine minor illnesses and
injuries, symptomatic care, minor trauma from physical training
or day-to-day base operations, and administration. The Algorithm-
Directed Troop Medical Care (ADTMC) guide is utilized for
sick call. Documentation takes place on Department of Army
Form 5181, Screening Note for Acute Medical Care, February
2003. Combat medics are trained to provide care with immediate
technical supervision from a physician or physician assistant.

116
CENTER FOR ARMY LESSONS LEARNED
The combat medic provides Tactical Combat Casualty Care
for operational casualties. Physicians and physician assistants
assigned to units are trained and equipped to provide advanced
trauma management.
• •
Hospitalization is provided at Level III and Level IV care by MTFs
staffed and equipped to provide care for all classes of patients by the
combat support hospital.
• •
Medical logistics encompasses Class VIII medical supplies and
equipment, medical equipment maintenance and repair support, optical
fabrication, medicinal gases, and blood and blood products. Medical
logistics is managed through the MEDLOG system.
• •
Preventive medicine services reduce the incidence of disease and
nonbattle injury. Signicant medical intelligence is collected by
preventive medicine planners to support the intelligence preparation of
the battleeld. They can be a good source of information regarding the
medical threat in the area of operations.
• •
Veterinary services provide support for food inspection, food safety
and security, surveillance and investigation of zoonotic disease or food
and waterborne illness, animal medical and surgical care, and civil-
military operations.
• •
Dental services provide operational care to avoid the loss of trained
manpower from dental disease or injury.
• •
Combat and operational stress control provides doctrinal guidance
for controlling excessive stress in combat and other operational
environments. Combat and operational stress control identies
command and leadership responsibilities and consultation, training,
and education assistance available for units. Many stressors in a
combat situation are due to deliberate enemy actions aimed at killing,
wounding, or demoralizing U.S. Soldiers and allies. Other stressors
are due to the operational environment. Some of these stressors can
be avoided or counteracted by wise command actions. Still, other
stressors are due to calculated or miscalculated choice, accepted in
order to exert greater stress on the enemy. Sound leadership works to
keep stressors within tolerable limits and prepares the troops mentally
and physically to endure them. Some of the most potent stressors can
be due to personal problems in the unit or on the home front. These,
too, must be identied and, when possible, corrected or controlled.
Unit needs assessments can help behavioral health providers identify
specic stressors in a unit and develop interventions to help unit
personnel cope.

117
TACTICAL COMBAT CASUALTY CARE HANDBOOK
• •
Medical laboratory support consists of limited facilities, equipment,
and personnel needed to analyze body tissues and uids to assist
in disease diagnosis and monitoring of therapy. The Special Forces
medical sergeant is highly trained in procedures such as microscopy
and utilizing point-of-care diagnostic analyzers that enhance the ability
to assess illness and injury.
• •
Medical command, control, and intelligence. At all levels of command,
a command surgeon is designated. This AMEDD ofcer is a special
staff ofcer charged with planning for and executing the Army Health
System (AHS) mission. At the lower levels of command, this ofcer
may be dual-hatted as an AHS unit commander. Further, he may
have a small staff section to assist him in planning, coordinating, and
synchronizing the AHS effort within the area of operations. Through
mission command, the command surgeon may be empowered to act
somewhat independently. However, the non-medical commander can
retain the authority to make decisions, which he feels are critical. To
be successful, mission command requires an environment of trust
and mutual understanding, which may be challenging to establish
for newly assigned staff members who have not had a previous
supporting relationship with the command. The command surgeon
is responsible for ensuring that all medical functions are considered
and included in running estimates, operation plans, and operation
orders. The command surgeon retains technical supervision of all AHS
operations. At the higher levels of command, the scope of duties and
responsibilities expand to include all subordinate levels of command.

119
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Appendix J
Tactical Combat Casualty Care Background
A study by COL Brian J. Eastridge, trauma consultant to the U.S. Army
Surgeon General, demonstrated that 87 percent of Operation Iraqi Freedom
(OIF) and Operation Enduring Freedom (OEF) combat deaths were
prehospital cases. Of these prehospital deaths, 24 percent were potentially
preventable, caused by extremity hemorrhage, airway obstruction,
junctional bleeding, truncal bleeding, or tension pneumothorax. This means
that more than 1,100 combat deaths potentially could have been prevented.
Guidance concerning Tactical Combat Casualty Care (TCCC) training in the
Services comes from the following sources:
• •
Assistant Secretary of Defense for Health Affairs (ASDHA)
Memorandum, 06 August 2009. The Defense Health Board advised
the ASDHA that all deploying Service members must receive
comprehensive training in TCCC.
• •
Defense Health Board, Combat Trauma Lessons Learned from
Military Operations of 2001-2013, 09 March 2015. “The survival
rate of Service members injured in combat has signicantly improved
during the recent decade of military conict due to advances in trauma
care and knowledge gained by medical personnel in the prehospital far
forward environment.”
• •
Bureau of Medicine and Surgery (BUMED) Instruction 1510.25,
07 May 2015. “All active duty and Reserve hospital corpsmen,
physician assistants, physicians, advanced practice nurses, and nurse
generalists shall complete TCCC training (to include the Expeditionary
Medicine Web-Based Training, if not already completed) within
180 days prior to each Individual Augmentee or Health Services
Augmentation program deployment or every 3 years in order to
maintain readiness. Completion of the full course of instruction
prior to each deployment will ensure the most up-to-date training is
received.”
• •
U.S. Air Force Surgeon General Memorandum 0771, Air Force
Surgeon General TCCC Letter, 21 August 2010. “Effective
immediately, all applicable Air Force training courses and programs
will incorporate the most current TCCC guidelines consistent with
their level of knowledge and prociency instruction related to
battleeld medical care.”

120
CENTER FOR ARMY LESSONS LEARNED
• •
Department of the Army Memorandum, 08 April 2010. “Recent
analysis revealed Soldiers in the ranks of E-5 and above are not
adequately trained in TCCC, nor are they familiar with the equipment
in the improved rst aid kit. ... We are pursuing to improve the
effectiveness of TCCC.”
• •
Defense Health Agency Education and Training (DHA E&T)
Directorate. A DHA E&T Directorate priority is the standardization of
TCCC training within the DOD.
• •
Joint Trauma System (JTS). The mission of the JTS is to improve
trauma care delivery and patient outcomes across the continuum of
care. The Committee on Tactical Combat Casualty Care (CoTCCC)
currently resides in the JTS.
• •
CoTCCC. Publishes and revises evidence-based guidelines, training,
slides, and videos. The TCCC-AC and TCCC-MP guidelines are
reviewed and updated by CoTCCC members.

121
TACTICAL COMBAT CASUALTY CARE HANDBOOK
Appendix K
References
Advanced Trauma Life Support Manual, Ninth Edition, American College
of Surgeons, Chicago, IL, September 2012.
Air Force Tactics, Techniques, and Procedures 3-42.71, Expeditionary
Medical Support (EMEDS) and Air Force Theater Hospital (AFTH), 27
August 2014.
All Army Activities (ALARACT) 355/2009, “Tactical Combat Casualty
Care Card for Point-Of-Injury Documentation,” Ofce of the Surgeon
General of the Army, ALARACT Message Date Time Group 242018Z
December 2009.
Army Regulation 40-68, Clinical Quality Management, 22 May 2009.
Army Techniques Publication (ATP) 4-02.2, Medical Evacuation, 12 August
2014.
ATP 4-02.5, Casualty Care, 10 May 2013.
ASDHA Memorandum to Services, “Tactical Combat Casualty Care,” 23
August 2011.
Assistant Secretary of Defense for Health Affairs (ASDHA), June 14,
2011, referencing the Defense Health Board (DHB) recommendations from
August 6, 2009.
Borden Institute, U.S. Army Medical Department Center and School,
Emergency War Surgery, Fourth Edition, Ofce of The Surgeon General,
United States Army, 2013.
Bureau of Medicine and Surgery (BUMED) Instruction 1510.25, Navy
Medicine Tactical Combat Casualty Care Program, 7 May 2015.
De La Cruz, J.P., J.J. Reyes, M.I. Ruiz-Moreno, et al. “Differences in the In
Vitro Antiplatelet Effect of Dexibuprofen, Ibuprofen, and Flurbiprofen in
Human Blood.” Anesthesia Analgesia. Volume 111, Issue 6, pages 1341-
1346, 2010.
Gerhardt, Robert T., Robert L. Mabry, Robert A. De Lorenzo, Frank K.
Butler, Chapter 3, “Fundamentals of Combat Casualty Care,” published in
Combat Casualty Care: Lessons Learned From OEF and OIF, Ofce of the
Surgeon General, United States Army, 2012.

122
CENTER FOR ARMY LESSONS LEARNED
Harris, M., R. Baba, R. Nahouraii, et al. “Self-Induced Bleeding Diathesis
in Soldiers at a FOB in South Eastern Afghanistan.” Military Medicine.
Volume 177, Issue 8, pages 928- 929, 2010.
Joint Publication (JP) 3-28, Defense Support of Civil Authorities, 31 July
2013.
JP 4-02, Health Service Support, 26 July 2012.
Kotwal, Russ S., et al., Saving Lives on the Battleeld: A Joint Trauma
System Review of Pre-Hospital Trauma Care in Combined Joint Operating
Area-Afghanistan (CJOA-A), United States Central Command, 30 January
2013.
Kotwal, Russ S., et al., Saving Lives on the Battleeld Part II — One Year
Later: A Joint Theater Trauma System and Joint Trauma System Review of
Pre-Hospital Trauma Care in Combined Joint Operating Area-Afghanistan
(CJOA-A), United States Central Command Joint Theater Trauma System-
Afghanistan, 30 May 2014.
Kragh, John F. Jr., “Use of Tourniquets and Their Effects on Limb Function
in the Modern Combat Environment,” Foot Ankle Clinic, Volume 15, Issue
1, March 2010.
National Association of Emergency Medical Technicians (NAEMT) Tactical
Combat Casualty Care Guidelines available online at http://www.naemt.org/
education/TCCC/guidelines_curriculum.
NAEMT, PHTLS: Prehospital Trauma Life Support Manual, 6th edition,
Mosby Inc., 2006.
Prehospital Trauma Life Support, Military Eighth Edition, Jones and
Bartlett Learning, November 2014.
Tactical Combat Casualty Care-Military Personnel Curriculum Update.
0102PP03A Tactical Combat Casualty Care-Military Personnel Tactical
Field Care No. 1, PowerPoint Presentation, 150603.
U.S. Army Training and Doctrine Command (TRADOC), “Assessment of
Tactical Combat Casualty Care,” 08 April 2010.

123
TACTICAL COMBAT CASUALTY CARE HANDBOOK
SUBMIT INFORMATION OR REQUEST PUBLICATIONS
To help you access information efciently, the Center for Army Lessons Learned (CALL)
posts publications and other useful products available for download on the CALL website:
http://call.army.mil
PROVIDE LESSONS AND BEST PRACTICES
OR SUBMIT AN AFTER ACTION REVIEW (AAR)
If your unit has identied lessons or best practices or would like to submit an AAR or a
request for information (RFI), please contact CALL using the following information:
Telephone: DSN 552-9569/9533; Commercial 913-684-9569/9533
Fax: DSN 552-4387; Commercial 913-684-4387
Mailing Address: Center for Army Lessons Learned
ATTN: Chief, Analysis Division
10 Meade Ave., Bldg. 50
Fort Leavenworth, KS 66027-1350
REQUEST COPIES OF CALL PUBLICATIONS
If you would like copies of this publication, please submit your request on the CALL
restricted website (CAC login required):
https://call2.army.mil
Click on “Request for Publications.” Please ll in all the information, including your unit
name and street address. Please include building number and street for military posts.
NOTE: Some CALL publications are no longer available in print. Digital publications
are available by clicking on “Publications by Type” under the “Resources” tab on the
CALL restricted website, where you can access and download information. CALL also
offers Web-based access to the CALL archives.
CALL produces the following publications on a variety of subjects:
Handbooks
Bulletins, Newsletters, and Observation Reports
Special Studies
News From the Front
Training Lessons and Best Practices
Initial Impressions Reports
FOLLOW CALL ON SOCIAL MEDIA
https://twitter.com/USArmy_CALL
https://www.facebook.com/CenterforArmyLessonsLearned

CENTER FOR ARMY LESSONS LEARNED
124
COMBINED ARMS CENTER (CAC)
Additional Publications and Resources
The CAC home page address is: http://usacac.army.mil
Center for Army Leadership (CAL)
CAL plans and programs leadership instruction, doctrine, and research. CAL integrates
and synchronizes the Professional Military Education Systems and Civilian Education
System. Find CAL products at http://usacac.army.mil/cac2/cal.
Combat Studies Institute (CSI)
CSI is a military history think tank that produces timely and relevant military history and
contemporary operational history. Find CSI products at http://usacac.army.mil/cac2/csi/
csipubs.asp.
Combined Arms Doctrine Directorate (CADD)
CADD develops, writes, and updates Army doctrine at the corps and division level. Find
the doctrinal publications at either the Army Publishing Directorate (APD) at http://
www.apd.army.mil or the Central Army Registry (formerly known as the Reimer Digital
Library) at http://www.adtdl.army.mil.
FMSO is a research and analysis center on Fort Leavenworth under the TRADOC G-2.
FMSO manages and conducts analytical programs focused on emerging and asymmetric
threats, regional military and security developments, and other issues that dene evolving
operational environments around the world. Find FMSO products at http://fmso.
leavenworth.army.mil.
Military Review (MR)
MR is a revered journal that provides a forum for original thought and debate on the art
and science of land warfare and other issues of current interest to the U.S. Army and the
Department of Defense. Find MR at http://usacac.army.mil/cac2/militaryreview.
TRADOC Intelligence Support Activity (TRISA)
TRISA is a eld agency of the TRADOC G-2 and a tenant organization on Fort
Leavenworth. TRISA is responsible for the development of intelligence products to
support the policy-making, training, combat development, models, and simulations arenas.
Capability Development Integration Directorate (CDID)
CDID conducts analysis, experimentation, and integration to identify future requirements
and manage current capabilities that enable the Army, as part of the Joint Force, to exercise
Mission Command and to operationalize the Human Dimension. Find CDID at http://
usacac.army.mil/organizations/mccoe/cdid.
Joint Center for International Security Force Assistance (JCISFA)
JCISFA’s mission is to capture and analyze security force assistance (SFA) lessons from
contemporary operations to advise combatant commands and military departments on
appropriate doctrine; practices; and proven tactics, techniques, and procedures (TTP) to
prepare for and conduct SFA missions efciently. JCISFA was created to institutionalize
SFA across DOD and serve as the DOD SFA Center of Excellence. Find JCISFA at https://
jcisfa.jcs.mil/Public/Index.aspx.
Support CAC in the exchange of information by telling us about your
successes so they may be shared and become Army successes.

